Article Text

Statistics from Altmetric.com
We note with interest and express our principle agreement with the views put forward by Professor Frederic Houssiau in the recent Editorial ‘Time to change the primary outcome of lupus trials’ published in Annals of the Rheumatic Diseases.1 Professor Houssiau advocated using steroid reduction as a primary outcome measure in systemic lupus erythematosus (SLE) clinical trials, or as a minimum, incorporating a steroid reduction target into the primary endpoint. This proposal was prompted by the observation that, like many other recent phase 3 clinical trials conducted with drugs that have a sound biological mechanism for benefit in SLE, the recently published CHABLIS-SC phase 3 clinical trial of subcutaneous blisibimod in SLE2 failed to meet its primary endpoint of a week 52-SLE Responder Index (SRI)-6. However, a significant steroid sparing effect was seen, with a modified endpoint of a week 52-SRI-6 combined with a reduction in steroid dose during weeks 40–52 compared with study entry, showing a trend to benefit for the blisibimod arm (23.3% of blisibimod-treated, compared with 14.3% of placebo-treatedpatients, p=0.056).
The harmful effects of long-term steroid use are well recognised, and there is specific evidence in SLE that steroids independently contribute to increased cardiovascular risk, osteoporotic fractures, avascular bone necrosis and diabetes mellitus.3 In addition, a number of studies have found that steroid exposure in SLE is associated with increased damage accrual,3 4 which is in turn associated with increased morbidity and mortality. Therefore, by extension, to be truly disease modifying, any SLE treatment should have a steroid sparing effect.
Last year, we published a systematic review and meta-analysis of steroid sparing effect of biological agents in phase 3 clinical trials in SLE that were published in the 10 years prior.5 Twenty-eight studies were identified; 9 conducted in SLE, 5 in lupus nephritis and 14 post hoc analyses of the original phase 3 trials in SLE. Of the eight drugs trialled in these studies (rituximab, belimumab, tabalumab, epratuzumab, atacicept, ocrelizumab, abetimus sodium and abatacept), only the BLISS-526 and BLISS-767 (intravenous belimumab), BLISS-SC8 (subcutaneous belimumab) and ILLUMINATE-29 (subcutaneous tabalumab) studies met their primary endpoints. However, effects on secondary endpoints including changes in serological markers were often seen, and a steroid reduction outcome measure was included in most, but not all, studies. As the steroid reduction endpoints reported in these studies were variable, to perform the meta-analysis of steroid sparing effect of these biological agents, we included the seven studies which reported a similar corticosteroid-reduction endpoint:
≤7.5 mg/day, and by ≥25% from baseline between weeks 40 and 52 (belimumab—BLISS-52,6 BLISS-767 and BLISS-SC8);
≤7.5 mg/day, between weeks 24 and 52 for ≥3 consecutive months, without increase in antimalarials/immunosuppressants (tabalumab—ILLUMINATE-110 and ILLUMINATE-29);
≤10 mg/day or ≤7.5 mg/day by week 24 (epratuzumab—ALLEVIATE-1 and ALLEVIATE-2, respectively11); or
<10 mg/day between weeks 24 and 52, with a major clinical response (rituximab—EXPLORER12).
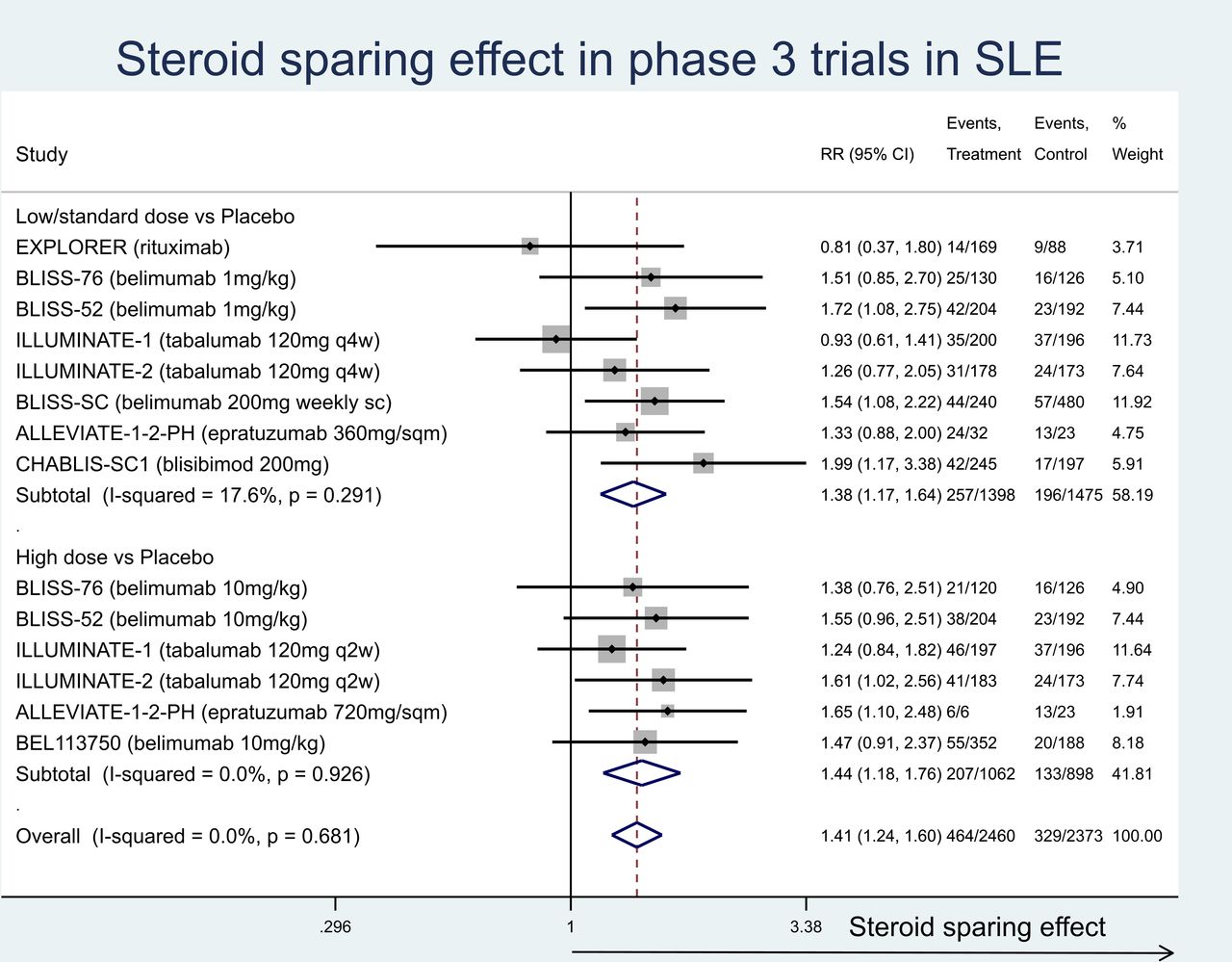
In this correspondence, we have updated our meta-analysis to include two additional phase 3 trials in SLE published since the systematic review—the CHABLIS-SC study,2 and the BEL113750 trial of intravenous belimumab 10 mg/kg conducted in China, South Korea and Japan.13 As noted above, the CHABLIS-SC study failed to meet its primary endpoint; however, the BEL113750 trial did meet its primary endpoint of a week 52-SRI-4 response (53.8% vs 40.1%, OR 1.99, p=0.0001). Similar to most other studies included in the meta-analysis (figure 1), both of these studies showed a reduction in steroids between weeks 40 and 52 to ≤7.5 mg/day, compared with placebo (17.2% vs 8.9%, p=0.019 for blisibimod, and 15.6% vs 10.9% for belimumab, p=0.0721).

{kind=link}
Meta-analysis of corticosteroid-sparing effect (expressed as relative risk) in phase 3 clinical trials of biological agents in systemic lupus erythematosus.
All measures of SLE disease activity (including composite endpoints, such as the SRI-4 and BICLA (BILAG-based combined lupus assessment), which are commonly used as primary outcome measures in SLE clinical trials) have inherent limitations, and it is evident from studies such as CHABLIS-SC that the choice of endpoint can have significant implications for the outcome of a clinical trial. We have shown in our meta-analysis that many of the biological agents that failed to show benefit in phase 3 clinical trials using composite endpoints, showed a steroid sparing effect. Given the importance of steroids in contributing to morbidity in SLE, we agree with Professor Houssiau that it is time to give strong consideration to including steroid sparing effect (captured as a dose reduction or a specific dose reached) in composite endpoints in SLE clinical trials.
Ethics statements
References
Footnotes
Handling editor Josef S Smolen
Contributors MN, SO and MH contributed conceptually to the drafting of this correspondence; SO wrote the response, MH performed the meta-analysis and all authors approved the final document.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.