Article Text

Statistics from Altmetric.com
We read with great interest the article by Minoia et al which named development and initial validation of the macrophage activation syndrome (MAS)/systemic juvenile idiopathic arthritis (sJIA) (MS) score for diagnosis of MAS in sJIA.
MAS is a life-threatening complication of rheumatic disorders, including sJIA, adult-onset Still’s disease (AOSD) and lupus.1–4 Timely diagnosis and appropriate treatment of MAS are particularly important to improve the prognosis of MAS patients. At present, hemophagocytic lymphohistiocytosis (HLH)-2004 and HLH-2009 criteria are widely used to identify MAS associated with AOSD. Hemophagocytic syndrome diagnostic (HS) score was developed previously to facilitate MAS recognition, but still requires validation.5 In 2019, Francesca Minoia et al reported a MS score for classification of sJIA-associated MAS patients.6 Considering that sJIA and AOSD are thought to constitute the same disease entity occurring at different ages, we intended to evaluate the application of MS score in AOSD-associated MAS patients.
We collected AOSD patients from 1 January 2012 to 31 July 2019 from six centres across China. Patients were included in this study if they were older than 18 years of age, and met the Yamagishi criteria for a diagnosis of AOSD. MAS was diagnosed using the HLH-2004 diagnostic criteria, and the diagnosis was confirmed by the attending rheumatologists. Clinical information was recorded and analysed. MS score was calculated for each patient according to the previous report.
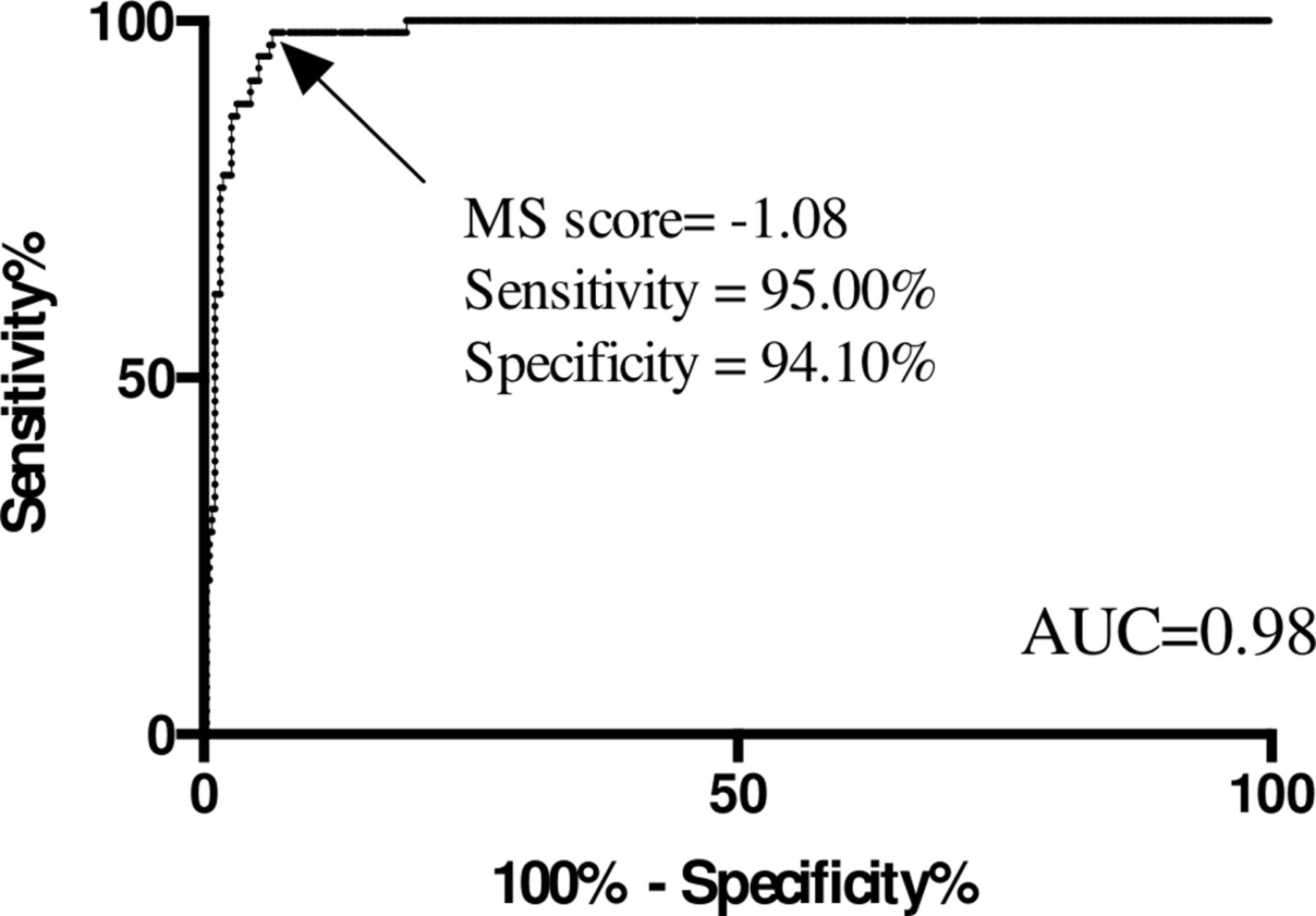
A total of 450 AOSD patients (60 AOSD associated MAS, 390 AOSD without MAS) were included in this study. Clinical features and lab results as the time of MAS diagnosis were shown in table 1. The application of the MS score (≥−2.1) yielded a sensitivity of 100%, a specificity of 29.85%, a positive predictive rate of 36.15%, a negative predictive rate of 100% in the diagnosis of AOSD-MAS with a Kappa value of 0.320. However, a further receiver operator characteristic curve analysis suggested that setting −1.08 as the score cut-off could provide the best discrimination between AOSD with and without MAS (figure 1). MS score ≥−1.08 yielded a sensitivity of 94.10%, a specificity of 95.00% in the diagnosis of MAS associated with AOSD. The positive predictive rate was 99.19% and the negative predictive rate of 71.25%, with a Kappa value of 0.781.

{kind=link}
Modified criteria of MS score in the diagnosis of AOSD associated MAS. In a febrile patient with AOSD, the diagnosis of MAS should be considered if the MS score is ≥-1.08. The area under the curve (AUC) of the model is 0.98. AOSD, adult-onset Still’s disease; MAS, macrophage activation syndrome.
Clinical manifestations of AOSD patients with and without MAS
The current finding suggested that even though there are many similarities between sJIA and AOSD, adult and young patients have notable differences in terms of clinical manifestations and lab results. For instance, central nervous involvement is quite rare in AOSD-MAS patients, probably because adults usually have much more stable central nervous system. In addition, the levels of platelet count and fibrinogen are usually lower in AOSD-MAS patients as compared with those in sJIA-MAS patients, which could lead to higher MS scores in AOSD patients. Therefore, the items calculated in the reported sJIA-MS score as well as the cut-off for sJIA-MAS diagnosis (>−2.1) should be modified for diagnosis of MAS associated with AOSD. In our cohort, MS score ≥−1.08 might be a better cut-off for AOSD-MAS diagnosis with an area under the curve of 0.98.
Further prospective and independent validations with larger sample size are needed to evaluate the modified MS score in the diagnosis for the life-threatening MAS condition in AOSD patients.
Ethics statements
Footnotes
Handling editor Josef Smolen
RW and TL contributed equally.
Correction notice This article has been corrected since it published Online First. The correspondence author details have been corrected.
Funding This study was funded by Science and Technology Commission of Shanghai Municipality.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.