Article Text

Abstract
Background Patients with inflammatory arthritidies have a higher cardiovascular (CV) risk than the general population. Traditional CV risk factors are involved, while the impact of the metabolic syndrome (MetS) is less defined. Whether MetS clinical presentation and its components are comparable across conditions is unclear.
Objectives To compare the prevalence of MetS and their components, and the impact on the CV risk profile, in psoriatic arthritis (PsA) versus rheumatoid arthritis (RA).
Methods a retrospective analysis with follow-up of real-world PsA (CASPAR criteria) and RA (2010 EULAR/ACR classification criteria) patients referred to a rheumatology clinic was performed. Demographical, clinical data and presence of CV risk factors were evaluated from patient charts using national guidelines, both at baseline and after 12-months of follow-up. MetS was defined according to the American Heart Association (AHA)/National Heart, Lung, and Blood Institute (NHLBI) criteria. Univariate and multivariate models were used to compare the impact of the MetS and its components in patients with PsA versus RA.
Results PsA patients (n=78) were younger (45.23 (16.99) vs 60.81 (13.19) years, p<0.001), exhibited lower disease duration (18.86 (48.43) vs 176 (169.77) months, p<0.001) and prevalence of autoantibodies (RF: 7.7 vs 58.7%, ACPA: 7.9 vs 57.6%; both p<0.001) than their RA counterparts (n=92). PsA patients were more likely to present with MetS (40(51.3%) vs 25(27.2%), p=0.003) and dyslipidemia (56(71.8%) vs 26(28.3%), p<0.001) compared to RA. No differences were observed for smoking (22(28.2%) vs 26(28.3%), p=0.836), diabetes (26(38.3%) vs 33(35.9%), p=0.823 and hypertension (44(56.4%) vs 51(55.4%), p=0.749). These differences were maintained after adjusting for age.
Multivariate analyses revealed that hypertension (OR 11.818 [95% CI: 2.046–58.053, p=0.002) and dyslipidemia (OR 5.190 [95% CI: 1.118–24.092], p=0.035) were predictors of MetS in PsA, and no effect was observed for diabetes (p=0.066) smoking (p=0.367), age (p=0.445) or sex (p=0.445); whereas diabetes (OR 15.58, [95% CI: 2.41–100.45], p=0.004), hypertension (OR 20.44, [95% CI: 2.58–161.05], p=0.004) and dyslipemia (OR 43.29 [95% CI: 6.82–274.75], p<0.001) predicted MetS in RA, and no effect of age (p=0.473), sex (p=0.615) or smoking (p=0.317) was noted. No effect was observed for autoantibodies or treatments received.
Despite the history of CV events was similar between disorders (PsA: 22(28.2%) vs RA 24(26.1%), p=0.602), differences in predictors were found. Multivariate analyses revealed that hypertension and MetS predicted CV history in PsA, whereas dyslipidemia was the only factor predicting CV history in RA (Table 1). Associations were stronger in PsA, and total variance explained in each model differed across groups.
Multivariate analysis of predictors of history of CV events in RA PsA and RA
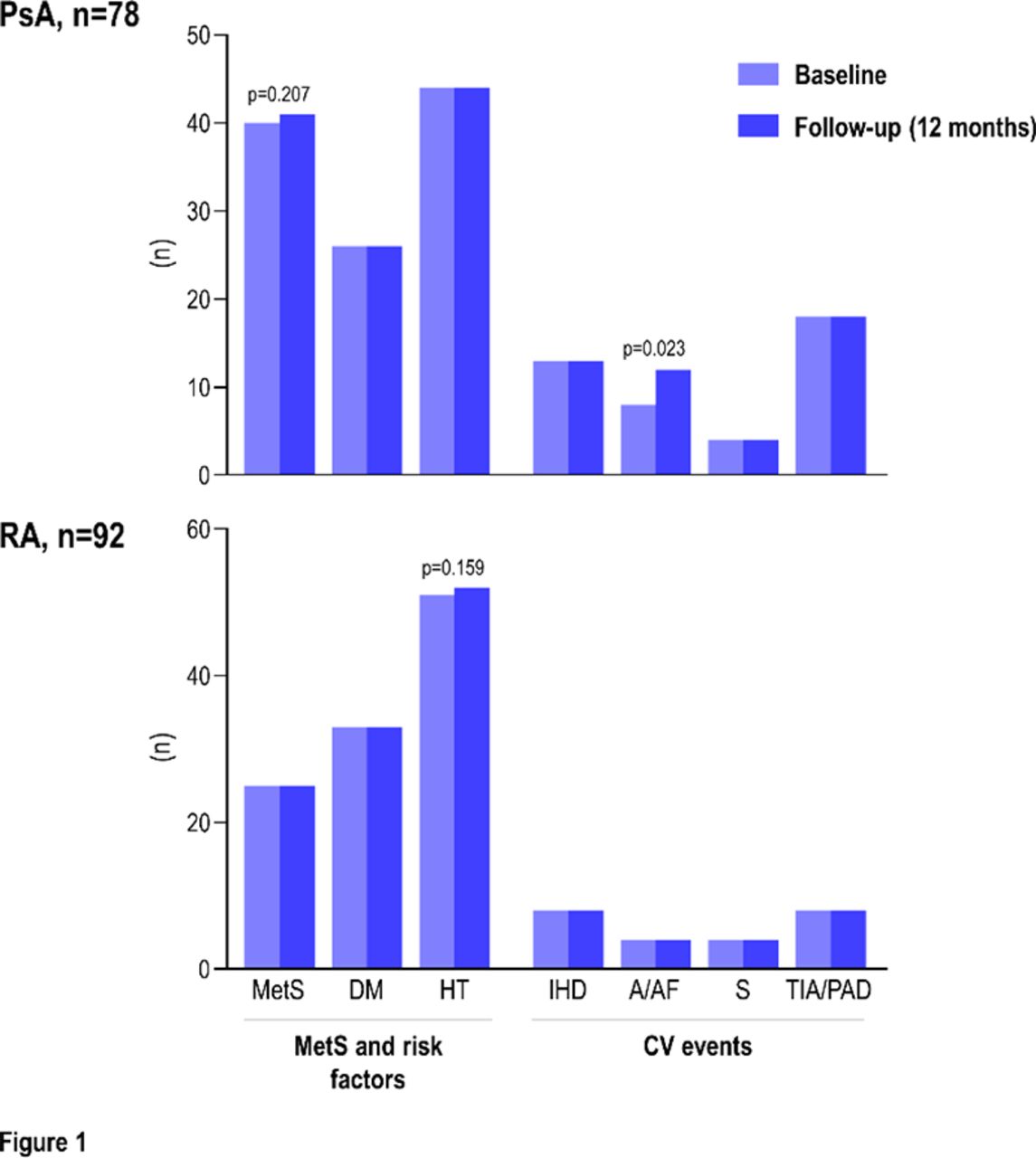
Finally, follow-up analyses revealed that progression of MetS and its components in PsA and RA were negligible after 12 months of follow-up (Figure 1).

{kind=link}
Conclusion Occurrence and presentation of MetS differed between inflammatory arthritidies. The impact of these risk factors on CV risk profile was stronger in PsA compared to RA, and showed no progression in one year. This suggests the implication of different mechanisms, which may require distinct CV preventive strategies in PsA and RA.
REFERENCES: NIL.
Acknowledgements: NIL.
Disclosure of Interests None Declared.
- Comorbidities
- Cardiovascular disease
- Inflammatory arthritides