Article Text

Abstract
Background Immune checkpoint inhibitor associated arthritis (ICI-A) commonly persists for months to years, even after ICI cessation.[1]
Objectives To compare the safety and effectiveness of biologic and conventional disease modifying anti-rheumatic drugs (DMARDs) for ICI-A.
Methods Retrospective multicenter observational study. Inclusion: 1) diagnosis of ICI-A and 2) treatment with a tumor necrosis factor inhibitor (TNFi), interleukin-6 receptor inhibitor (IL6Ri) and/or methotrexate (MTX). Exclusion: preexisting autoimmune disease. The primary outcome was time to cancer progression from ICI initiation. Patients whose cancer progressed prior to DMARD initiation were excluded from this analysis. The secondary outcome was time to arthritis control from DMARD initiation, defined as grade 1 arthritis and prednisone ≤10mg/day. Cox proportional hazard models were generated, adjusting for confounders. A sensitivity analysis was performed incorporating a time dependent variable “time from ICI initiation to DMARD initiation.”
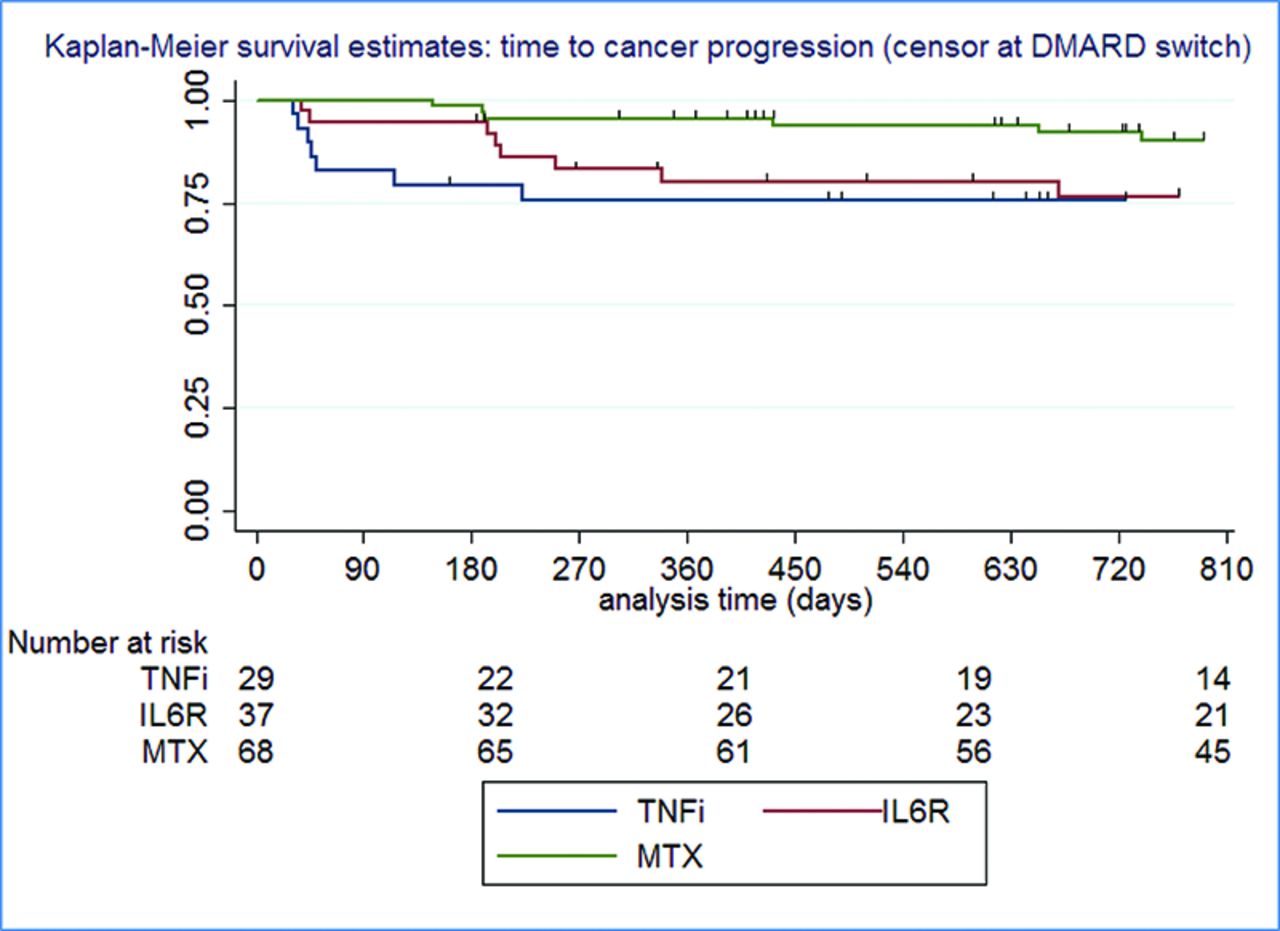
Results 147 patients were included, mean (SD) age 60.3 (11.9) years, 66 (45%) females. Sixty percent had received PD1/PDL1 monotherapy, 30% received combination CTLA4/PD1. Eighty percent had stage IV cancer. ICI-A treatment was TNFi in 33 (22%), IL6Ri 42 (29%), MTX 72 (49%) (Table 1). A Kaplan-Meier curve showing time to cancer progression by DMARD is shown in Figure 1. In an unadjusted Cox model with MTX as the reference, time to cancer progression with a TNFi was HR 2.51 (95% CI 0.91-6.93, p=0.075) and for IL6Ri HR 2.36 (95% CI 0.91-6.12, p=0.078). After adjustment for the time dependent variable, time to cancer progression was significantly shorter for TNFi-treated patients compared to MTX, HR 3.27 (95% CI 1.21-8.84, p=0.019). The result for IL6Ri was HR 2.31 (95% CI 0.98-5.41, p=0.055). Time to arthritis control was significantly faster for TNFi compared to MTX, HR 1.91 (95% CI 1.06-3.45, p=0.032) in an adjusted Cox model. Results for IL6Ri were HR 1.66 (95% CI 0.93-2.97, p=0.089). Results for cancer progression and arthritis control were similar in the subset of patients with melanoma.
Conclusion Treatment of ICI-A with biologic DMARDs is associated with more rapid arthritis control than with MTX but may be associated with a shorter time to cancer progression. A prospective randomized controlled trial is needed to verify these findings and to identify the optimal approach to managing patients with high grade ICI-A.
Reference [1] Braaten TJ, et al Ann Rheum Dis. 2020 Mar;79(3):332-338.
Patient characteristics

{kind=link}
Kaplan-Meier curve showing time to cancer progression from time of immune checkpoint inhibitor initiation
Acknowledgements: NIL.
Disclosure of Interests Anne Bass: None declared, Noha Abdel-Wahab Speakers bureau: ChemoCentryx, Consultant of: ChemoCentryx, Pankti Reid: None declared, Jeffrey Sparks Consultant of: Bristol Myers Squibb, AbbVie, Amgen, Boehringer Ingelheim, Gilead, Inova Diagnostics, Janssen, Optum, Pfizer, Grant/research support from: Bristol Myers Squibb, cassandra calabrese Speakers bureau: Sanofi, Consultant of: Astazenica, Deanna Jannat-Khah: None declared, Nilasha Ghosh: None declared, Divya Rajesh: None declared, Carlos Aude: None declared, Lydia Gedmintas: None declared, Lindsey MacFarlane: None declared, Senada Arabelovic: None declared, Adewunmi Falohun: None declared, Komal Mushtak: None declared, Farah Al Haj: None declared, Adi Diab: None declared, Ami Shah Grant/research support from: Eicos Sciences, Medpace LLC, Arena Pharmaceuticals, Kadmon Corporation, Clifton Bingham Consultant of: Bristol Myers Squibb,: Abbvie, Janssen, Lilly, Pfizer, Sanofi, Moderna, Grant/research support from: Bristol Myers Squibb, Karmela Kim Chan: None declared, Laura Cappelli Consultant of: Bristol Myers Squibb, Grant/research support from: Bristol Myers Squibb.
- Malignancy
- bDMARD
- Inflammatory arthritides