Article Text

Abstract
Objectives To compare all-cause mortality and causes of death between patients with psoriatic arthritis (PsA) and the general population in Sweden.
Methods Adults with at least one main PsA diagnosis (International Classification of Diseases-10: L40.5/M07.0–M07.3) from outpatient rheumatology/internal medicine departments 2001–2017 were identified from the National Patient Register. Each case was matched to five population comparator-subjects on sex/county/age at the case’s first arthritis diagnosis. Follow-up ran from 1 January 2007, or from first PsA diagnosis thereafter, until death, emigration or 31 December 2018. Mortality was assessed overall, and stratified by sex and duration since diagnosis (diagnosis before/after 1 January 2007), using matched Cox proportional hazard regression (excluding/including adjustments for comorbidity) or Breslow test, as appropriate. Incidence rate ratios (IRR) of death, overall and stratified by sex/duration since diagnosis/age, as well as causes of death in PsA cases and comparator-subjects were also described.
Results All-cause mortality was elevated in PsA (HR: 1.11 (95% CI: 1.07 to 1.16); IRR: 1.18 (95% CI: 1.13 to 1.22)), mainly driven by increased risks in women (HR: 1.23 (95% CI: 1.16 to 1.30)) and cases with longer time since diagnosis (HR: 1.18 (95% CI: 1.12 to 1.25)). IRR of death were significantly increased for all ages except below 40 years, with the numerically highest point-estimates for ages 40–59 years. When adjusted for comorbidity, however, the elevated mortality risk in PsA disappeared. Causes of death were similar among PsA cases/comparator-subjects, with cardiovascular disease and malignancy as the leading causes.
Conclusions Mortality risk in PsA in Sweden was about 10% higher than in the general population, driven by excess comorbidity and with increased risks mainly in women and patients with longer disease duration.
- Arthritis, Psoriatic
- Epidemiology
- Mortality
- Cause of Death
- Sweden
Data availability statement
Data may be obtained from a third party and are not publicly available. The study was conducted using de-identified participant data from various national Swedish administrative and healthcare registers. For further information the corresponding author JKW (johan.81.karlsson@gmail.com) may be contacted.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Psoriatic arthritis, as other chronic inflammatory diseases, such as rheumatoid arthritis, ankylosing spondylitis and psoriasis, is associated with elevated risks for a number of different comorbidities, including cardiovascular disease. However, in contrast to the increased mortality reported in the other conditions, prior mortality estimates in psoriatic arthritis have been inconsistent.
WHAT THIS STUDY ADDS
In this nationwide Swedish study, the largest assessment to date anywhere regarding mortality in psoriatic arthritis (assessing more than 33 000 patients for up to 12 years), the all-cause mortality was elevated by around 10% as compared with the general population, mainly driven by increased risks among women and patients with longer duration since diagnosis, and emanating from an excess comorbidity burden. The distributions of causes of death were, however, similar between patients and population comparator-subjects.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Considering the advances in the diagnosis and treatment of psoriatic arthritis, contemporary, nationwide mortality estimates, as well as identification of predictors and leading causes of death, are important to enable prevention of premature mortality.
Introduction
Psoriatic arthritis (PsA) is an inflammatory arthritic disease, associated with psoriasis (PsO). Similar to several other chronic inflammatory diseases, such as rheumatoid arthritis (RA) and ankylosing spondylitis (AS),1–5 PsO and PsA are both associated with an elevated burden of traditional cardiovascular disease (CVD) risk factors, increased subclinical atherosclerosis and a higher prevalence of manifest CVD.4 6–12 Beyond this, several other conditions, including infections and depression, as well as the extra-musculoskeletal manifestations uveitis and inflammatory bowel disease (IBD), are also more common in PsA than in the general population.13 14
Although RA and AS are both associated with increased all-cause mortality,15–20 in PsA the available data regarding mortality are conflicting.21–35 Many of these, at least seemingly contradictive, prior estimates are derived from hospital-based, single centre cohorts or smaller population-based assessments, but even when focusing on larger, population-based studies (including around 5000–20 000 PsA cases), some report an increased all-cause mortality in PsA,29 30 33 while others do not.18 27 35 36 In a recent meta-analysis, all-cause mortality in the overall PsA population was not found to be elevated (risk ratio: 1.12 (95% CI: 0.96 to 1.30)).19 A sex difference was observed, however, with a significantly increased mortality risk among female patients (risk ratio: 1.19 (95% CI: 1.04 to 1.36)).19 Meanwhile, PsO has been more consistently associated with an elevated mortality risk, which also appears to increase with more severe skin involvement.27 36 37
In light of these conflicting data, the current nationwide, population-based study aimed to compare all-cause mortality between patients with PsA and matched general population comparator-subjects in Sweden, overall as well as stratified by sex and duration since diagnosis. Secondary objectives were to describe the cause of death distributions among patients with PsA and comparator-subjects, and to investigate socioeconomic and disease-related mortality predictors.
Methods
Study setting and data sources
This is a nationwide, population-based cohort study of all-cause mortality in patients with PsA and matched general population comparator-subjects, using linked (via the personal identification number, unique to every permanent resident in Sweden), prospectively collected data from high-quality, nationwide, Swedish administrative and healthcare registers. In Sweden, PsA is typically diagnosed and treated in specialised outpatient care, normally at rheumatology or internal medicine departments.38 However, milder cases without need of disease-modifying anti-rheumatic drug (DMARD) therapy may be referred back to primary care after the initial diagnosis.
Administrative data, including International Classification of Diseases (ICD) diagnostic codes and dates, from inpatient and specialised (non-primary) outpatient care are recorded in the Swedish National Patient Register (NPR).39 Inpatient care data are available since 1964, with complete national coverage from 1987. The outpatient part of the NPR was started in 2001. Its coverage is now nearly complete, although missing information from some private caregivers.40 From each healthcare episode/visit, one main and, optionally, secondary diagnostic codes are recorded (using the Swedish versions of ICD-7: 1964–1968; ICD-8: 1968–1986; ICD-9: 1987–1996; ICD-10: 1997-present), as are any procedural-codes for surgery, etc. For the present study, ICD-codes from the NPR were used to identify PsA cases, and ICD-codes and procedural-codes to assess comorbidities (online supplemental tables S1 and S2).
Supplemental material
Prescription drugs dispensed by Swedish pharmacies are since 2005 registered in the Prescribed Drug Register (PDR), with a near 100% coverage.41 42 For the current study, PDR data were used to describe anti-rheumatic drug use, and as a complement to the NPR for identification of certain comorbidities (online supplemental table S3). Data on intravenous DMARDs administered in-hospital, which are not captured in the PDR, were retrieved by combining information from the PDR and the Swedish Rheumatology Quality Register.43
General population comparator-subjects were identified from the Total Population Register at Statistics Sweden, which was also the source of information on descent, immigration, emigration, residency and level of formal education.44
The primary outcome, all-cause mortality, as well as causes of death, were assessed using data from the Cause of Death Register, containing information on date and cause of death (according to ICD-codes; online supplemental table S1) for all deceased residents in Sweden since 1961.45
Study population and follow-up
All individuals in Sweden, having received at least one main diagnosis of PsA (ICD-10: L40.5/M07.0/M07.1/M07.2/M07.3) from outpatient visits to rheumatology or internal medicine departments at age 18 years or more (PsA index case definition) during 2001–2017, were identified from the NPR. Subjects who had received ICD-codes for PsA exclusively from inpatient care were not included, as PsA in Sweden is typically diagnosed and managed in specialised outpatient care, and a prior study also showed a high validity of our case definition, with 86% fulfilling established PsA classification criteria.46 For each PsA case, five general population comparator-subjects were randomly identified, matched on sex, county and age at first registered arthritis diagnosis for the index case. Matching at first arthritis, rather than PsA, diagnosis was chosen as some cases were expected to first receive another arthritis diagnosis, before characterisation as PsA.
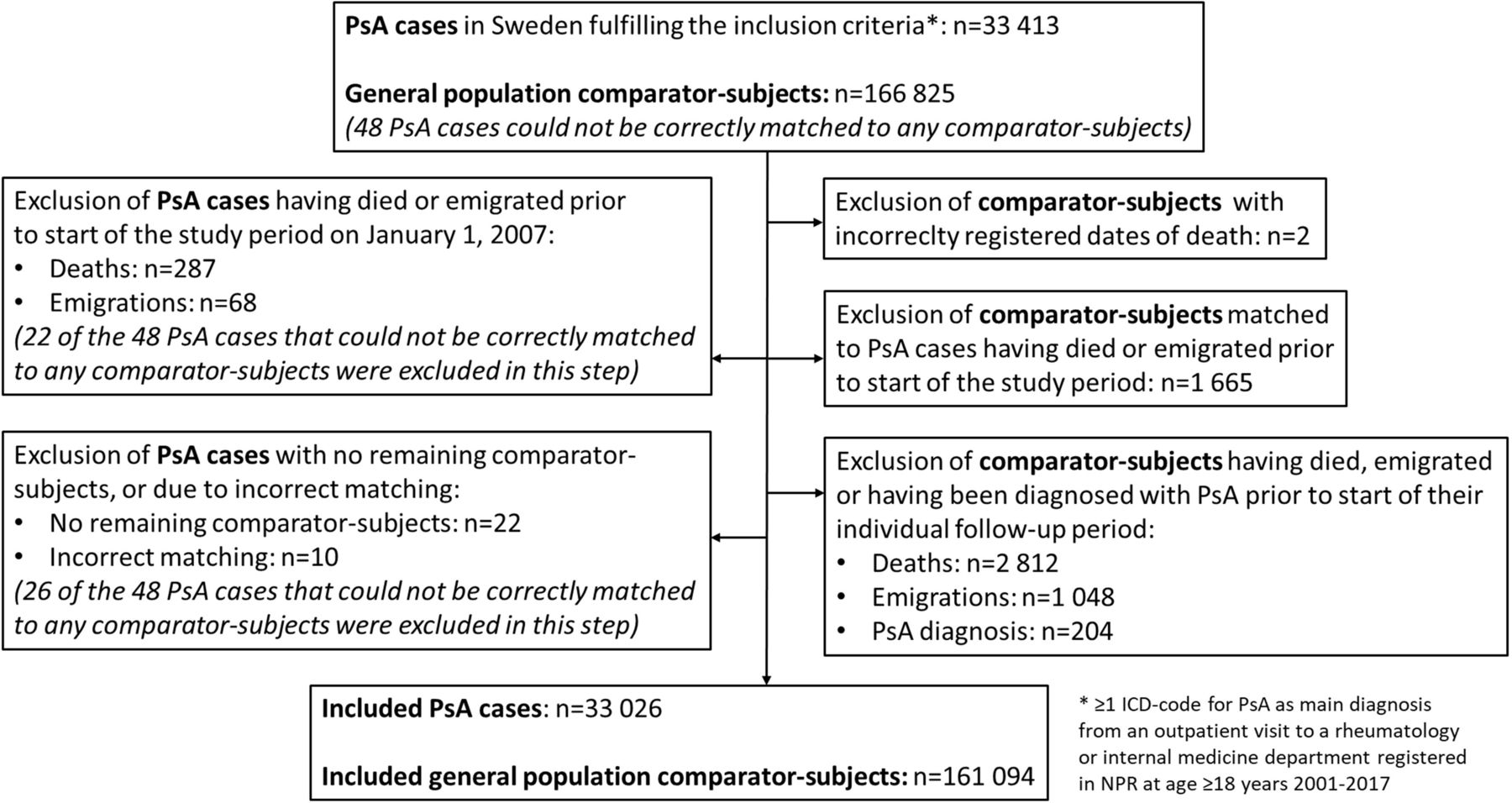
The date each PsA case fulfilled the index case definition (see above) served as their index date. PsA cases were followed from 1 January 2007, if their index date was prior to this, or from the index date if later, until death, emigration or end of the study on 31 December 2018. Comparator-subjects’ assessment period started simultaneously with their index case. PsA cases that died or emigrated before the start of the study period on 1 January 2007 were excluded together with their matched comparator-subjects. Comparator-subjects who died, emigrated or were themselves diagnosed with PsA before the start of their individual assessment periods were also excluded, but their respective index cases retained, as long as at least one of their five comparator-subjects could be included. Comparator-subjects diagnosed with PsA during follow-up served as comparator-subjects until receiving their first ever ICD-code for PsA (main/secondary diagnosis from any department), and thereafter (if meeting the PsA index case definition) as PsA cases with their own matched comparator-subjects. Figure 1 describes the study inclusion (final study population: 33 026 PsA cases and 161 094 comparator-subjects).

Inclusion flow chart. ICD, International Classification of Diseases; NPR, National Patient Register; PsA, psoriatic arthritis.
Outcomes
The primary outcome was all-cause mortality among the PsA cases in relation to comparator-subjects. Matched comparisons were conducted overall, as well as stratified for sex and duration since PsA diagnosis (as a surrogate marker for disease duration; index date prior to 1 January 2007 (‘longer duration since diagnosis’/prevalent cases) vs index date 2007–2017 (‘newly diagnosed cases’)). Furthermore, crude mortality rates (MR) and incidence rate ratios (IRR) of death between PsA cases and comparator-subjects were calculated overall and stratified for sex, age-intervals and duration since PsA diagnosis. Since PsA is associated with increased risks for various other diseases,4 9 10 13 14 and since patients will not die from the arthritis itself, in our main analyses we did not adjust the mortality estimates for comorbidity status, arguing that analyses without such adjustments will better capture the full impact of PsA on mortality. However, in order to explore the influence of measurable comorbidities, potentially related to PsO/PsA, on mortality, we also conducted an additional analysis including such adjustments (for the overall comparison between PsA cases and comparator-subjects).
As a secondary outcome, cause of death frequencies in PsA cases and comparator-subjects, based on the underlying cause of death registered in the Cause of Death Register, were described, divided into eight categories. Finally, potential socioeconomic and health-related predictors (extra-musculoskeletal manifestations, general comorbidities, surgery, present/diagnosed prior to start of follow-up) of increased mortality within the PsA group were investigated and related to the corresponding estimates among the comparator-subjects.
Statistics
All-cause mortality was visualised by Kaplan-Meier curves and compared by Cox proportional hazard regression analyses, accounting for the matched design. In case the Cox proportionality assumptions did not hold (as evaluated graphically in Kaplan-Meier curves and by log-minus-log plots), matched Breslow test was used instead. Estimated time to 10% mortality was described for all analyses to enhance comparability. While our main analyses were unadjusted for comorbidity status, in an additional analysis adjustments for education (>12 vs ≤12 years) and the presence of general comorbidities prior to start of follow-up (CVD, diabetes mellitus, infection (any; see table 1), chronic pulmonary disease, chronic kidney disease, malignancy, anxiety and depression; all yes/no, assessed as described in table 1) were added to the matched Cox proportional hazard regression, comparing all-cause mortality between PsA cases and comparator-subjects.
Demographics and disease characteristics of the psoriatic arthritis and comparator-subject cohorts at start of follow-up
Crude total, age-interval-specific, sex-specific and duration from diagnosis-specific MR for PsA cases and comparator-subjects were expressed as the number of deaths per 1000 person-years (PY) at risk, and the respective IRR with 95% CI (Byar method).
Mortality predictors at start of follow-up among the PsA cases were assessed by separate Cox proportional hazard regression models, adjusted for sex and age (or in case of violation of the Cox proportionality assumptions matched Breslow test). For comparability, the same analyses were also conducted separately among comparator-subjects. In the entire material (ie, including both PsA and comparator-subjects) we moreover assessed whether the interaction terms between the PsA case/comparator-subject status and the assessed predictors were significant, indicating a difference of the predictive ability in the two groups. Variables that were significantly associated with mortality in PsA in these analyses were then further examined in multivariate Cox proportional hazard regression analyses in PsA and comparator-subjects, respectively, again including an assessment of interaction terms in the entire material.
Sensitivity analyses
In relation to the primary outcome assessment, a number of sensitivity analyses were performed to account for: (1) potential misclassification of PsA diagnoses among the cases; (2) that an increased mortality may be expected during the first months after diagnosis of a disease; (3) potential survivorship bias due to the possible time-lag between the matching of comparator-subjects to PsA cases and the start of the individual assessment period (see Study population and follow-up above). The sensitivity analyses are described in greater detail in the online supplement.
Patient and public involvement
A patient research partner (see Acknowledgements) was involved in the research group and took part in discussions of the current results.
Results
Study population characteristics
The study population consisted of 33 026 PsA cases and 161 094 comparator-subjects (figure 1). For 90% of PsA cases, all five matched comparator-subjects could be included, while only 1.8% entered the analyses with three or fewer comparator-subjects. At the start of their individual follow-up, the PsA cases had a mean (SD) age of 52 (14) years and 45% were men (table 1). Regarding duration since PsA diagnosis, 12 568 (38%) cases had been diagnosed prior to the start of the study period at 1 January 2007 (thus constituting the longer duration since PsA diagnosis subset/prevalent cases). All assessed comorbidities were numerically more frequent among PsA cases than comparator-subjects at the start of follow-up (table 1). Anti-rheumatic therapy at start of and during follow-up is described in table 1 and online supplemental table S5, respectively, while online supplemental table S4 displays characteristics of the PsA cases and comparator-subjects stratified for sex.
All-cause mortality
During the 12-year study period (2007–2018), PsA cases and comparator-subjects were followed for a median (IQR) 8.8 (7.1) and 8.8 (7.2) years, respectively, contributing a total of 268 383 and 1 302 152 PY at risk. Over this period, 3121 deaths (9.4%) occurred among the PsA cases and 12 883 deaths (8.0%) among the comparator-subjects, while 312/2858 PsA cases/comparator-subjects were censored due to emigration and 525 comparator-subjects due to themselves being diagnosed with PsA.
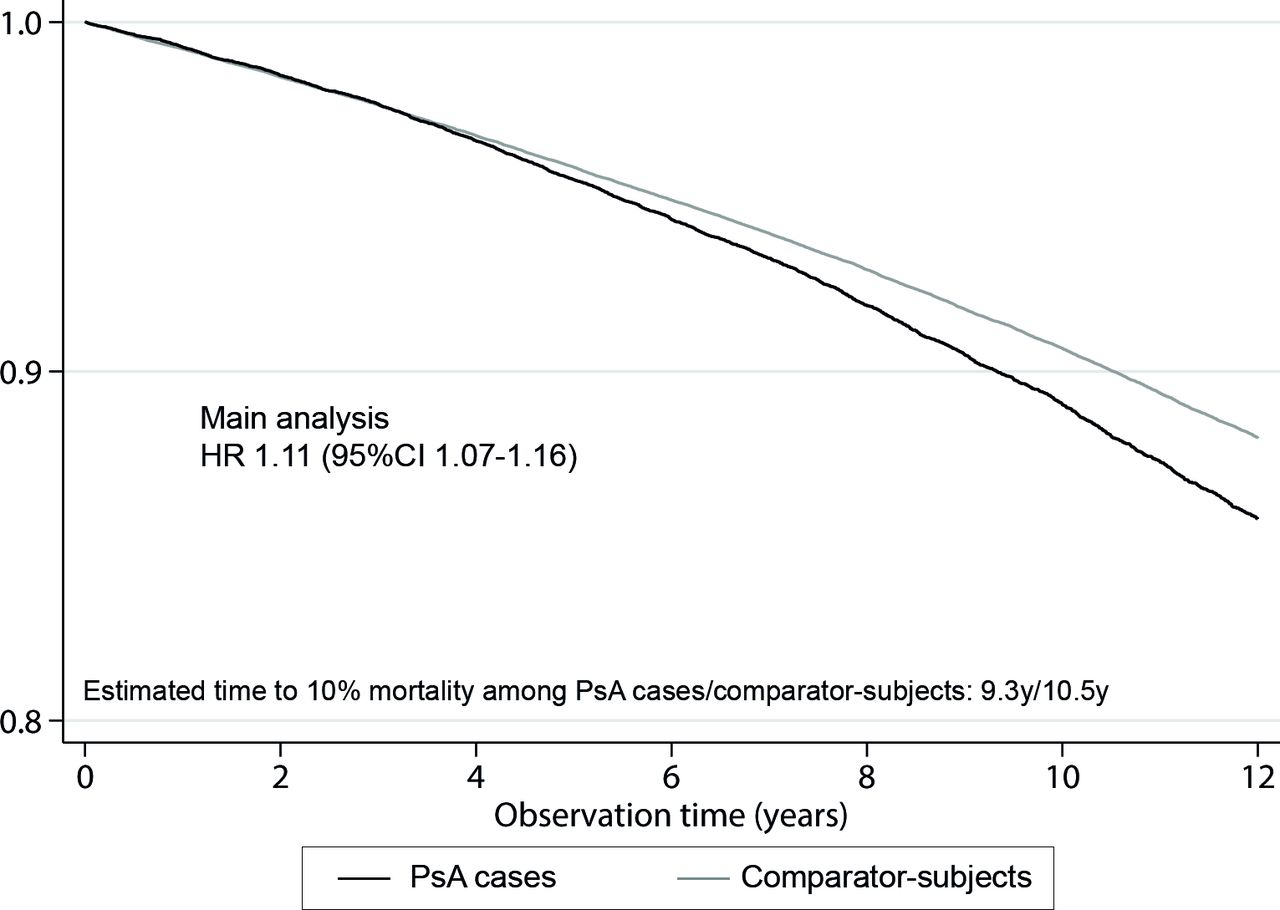
In the main analysis, this resulted in a significantly increased all-cause mortality among the PsA cases in relation to comparator-subjects (HR: 1.11 (95% CI: 1.07 to 1.16), figure 2; crude IRR: 1.18 (95% CI: 1.13 to 1.22), table 2). All sensitivity analyses also gave results in line with this (online supplemental file 1). After adjustment for comorbidities, however, PsA was no longer associated with an increased all-cause mortality (HR: 0.96 (95% CI: 0.92 to 1.01)), indicating that it is the excess comorbidity burden in the patients with PsA that drives the elevated mortality risk.

Comparison of all-cause mortality between patients with psoriatic arthritis in Sweden and matched general population comparator-subjects. Kaplan-Meier survival curves and matched Cox proportional HR, comparing all-cause mortality among PsA cases (n=33 026) to that of general population comparator-subjects, matched for sex, age and county (n=161 094), in Sweden 2007–2018. PsA, psoriatic arthritis; y, years.
Mortality rates and incidence rate ratios of death between the psoriatic arthritis cases and comparator-subjects in total and by sex, age and disease duration
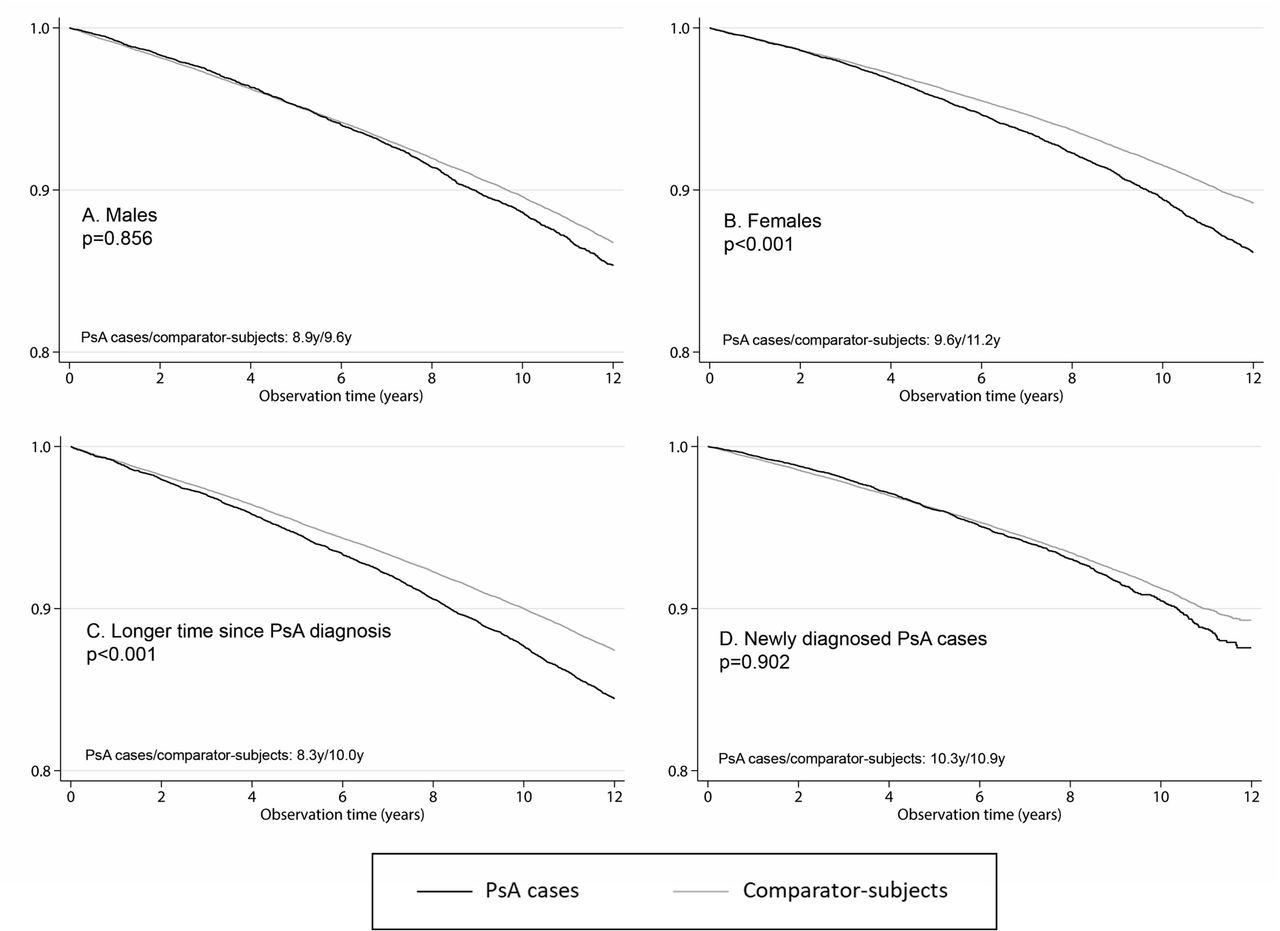
On stratification, the increased mortality in our main analysis was seen to mainly emanate from female PsA cases and PsA cases with longer duration since diagnosis, respectively (figure 3; table 2). Overall, as well as for female PsA cases, the crude IRRs of death were significantly increased during all age-intervals except below 40 years, with the numerically highest point-estimates at ages 40–49 and 50–59 years (table 2). There were similar, but weaker and non-significant age-trends among men.

{kind=link}
{kind=link}
{kind=link}
Comparison of all-cause mortality between patients with psoriatic arthritis in Sweden and matched general population comparator-subjects, stratified for sex and duration since PsA diagnosis. Kaplan-Meier survival curves, comparing all-cause mortality between PsA cases and general population comparator-subjects, matched for sex, age and county, in Sweden 2007–2018, stratified for sex and duration since PsA diagnosis. Estimated time to 10% mortality displayed below the curves. (A) 15 004 male PsA cases versus 73 060 male comparator-subjects; p=0.856 for the between-group comparison by matched Breslow test. (B) 18 022 female PsA cases versus 88 034 female comparator-subjects; HR: 1.23 (95% CI: 1.16 to 1.30) for the between-group comparison by matched Cox proportional hazard regression. (C) 12 568 prevalent PsA cases diagnosed prior to start of the study period on 1 January 2007 versus their 60 190 comparator-subjects; HR: 1.18 (95% CI: 1.12 to 1.25) by matched Cox proportional hazard regression. (D) 20 458 newly diagnosed PsA cases (ie, diagnosed 2007–2017) versus their 100 904 comparator-subjects; p=0.902 for the between-group comparison by matched Breslow test. PsA, psoriatic arthritis; y, years.
Causes of death
Causes of death were overall similarly distributed between PsA cases and comparator-subjects, with CVD and malignancies being the leading causes in both cohorts. Numerically a slightly higher percentage of PsA cases than comparator-subjects died from causes other than malignancies (71% vs 66%; table 3).
Causes of death* in the psoriatic arthritis and comparator-subject cohorts, in total and stratified for sex
Predictors of mortality
Lower socioeconomic status (using education level as proxy), prior joint surgery (which in PsA may reflect more severe disease, at least in prevalent cases) and presence of all assessed general comorbidities at the start of follow-up were significant predictors of mortality among both PsA cases and comparator-subjects in the sex- and age-adjusted analyses (table 4). Extra-musculoskeletal manifestations, that is, uveitis and IBD, did not predict mortality in PsA (estimated time to 10% mortality among PsA cases with/without prior anterior/posterior uveitis was 9.3/9.3 years, p=0.568 by Breslow test and for PsA cases with/without IBD 8.3/9.3 years, p=0.277 by Breslow test), while IBD, but not uveitis, was associated with increased mortality among the comparator-subjects (adjusted HR: 1.25 (95% CI: 1.07 to 1.45) for IBD; 0.98 (95% CI: 0.82 to 1.17) for uveitis).
Predictors at start of follow-up of mortality among PsA cases and comparator-subjects
Apart from the differing results regarding IBD, differences in the predictive abilities between the PsA and comparator-subject cohorts, as demonstrated by significant interactions, were only observed for prior hip and/or knee replacement surgery, which was a stronger mortality predictor in PsA, and for comorbid malignancy or anxiety/depression, both stronger mortality predictors in comparator-subjects (table 4). The multivariate predictor analyses rendered similar results, although without a between-group difference in the predictive ability of comorbid malignancy (online supplemental table S6).
Discussion
Main findings
In this large, nationwide, population-based, 12-year, cohort study (PsA cases, n=33 026), the all-cause mortality risk in patients with PsA diagnosed in specialised rheumatology/internal medicine care in Sweden was significantly increased, although only by around 10%, compared with the general population, mainly driven by increased risks in women and patients with longer duration since PsA diagnosis. When adjusting for comorbidity status, the increased mortality risk disappeared, indicating that the excess comorbidity burden in PsA (whether causally related to PsO/PsA or not) is the driving force behind the elevated mortality. The cause of death distributions were similar between PsA cases and comparator-subjects, with CVD and malignancy being the leading causes of death in both groups. Predictors of mortality were also generally similar in both cohorts (lower socioeconomic status, general comorbidities, prior joint surgery), although IBD did not predict mortality in PsA and hip/knee replacement surgery was a stronger mortality predictor in PsA than in the general population.
Previous research
Many of the contradictive, prior mortality estimates in PsA derive from hospital-based, single centre cohorts or smaller population-based studies (with fewer than 1000 PsA cases; online supplemental table S7). Considering that hospital-based studies are likely to capture patients with more severe disease compared with population-based cohorts, mortality estimates from such assessments may be expected to be inflated. However, even the results of these studies are inconsistent in observing an elevated mortality risk in PsA or not (online supplemental table S7). Turning to larger population-based assessments, two studies from Taiwan (9572 patients, 2001–2012, and 8795 patients, 2000–2012) demonstrated a standardised mortality ratio (SMR) of 1.47 (95% CI: 1.36 to 1.58) and HR of 1.52 (95% CI: 1.39 to 1.66), respectively.29 30 Furthermore, the SMR was also increased at 1.34 (95% CI: 1.16 to 1.52) in a Canadian study (15 430 patients, 1996–2016).33 On the other hand, large population-based studies from the UK (8706 patients, 1994–2010),27 Denmark (9817 patients, 1998–2014),36 Israel (5275 patients, 2003–2018)35 and Norway (18 700 patients, 2010–2017),18 did not demonstrate an increased mortality risk in PsA, with reported HR of 1.02 (95% CI: 0.92 to 1.12), stratified HR of 1.06 (no CI reported) and adjusted HR of 1.02 (95% CI: 0.90 to 1.15) and 1.06 (95% CI: 0.99 to 1.13), respectively. This diversity of results was also highlighted in a recent meta-analysis, wherein no increased all-cause mortality in the overall PsA population was found (relative risk 1.12 (95% CI: 0.96 to 1.30)), although the point estimate was very similar to that found in the present study (and an increased risk was indeed observed among female patients with PsA, see below).19 In the aforementioned Israeli cohort, the final, non-increased mortality estimate was adjusted for comorbidities, whereas their crude assessment did show an elevated HR in line with ours at 1.16 (95% CI: 1.04 to 1.29).35 Aiming to quantify the total impact of PsA and its associated comorbidities on mortality, in our main analyses we did not adjust our morality estimates for comorbidities, as we consider this to better illustrate the real burden of PsA. As expected, however, when including such adjustments in an additional analysis, the elevated mortality risk associated with PsA disappeared.
In women with PsA, we found the all-cause mortality risk relative to their sex-matched comparator-subjects to be higher than in male patients, although with lower absolute MR. This observation is in line with the above mentioned meta-analysis,19 as well as the recently published Norwegian study,18 both of which (similar to us) found a significantly increased mortality risk among female, but not male, patients with PsA. To establish the reasons behind this sex difference was beyond the scope of the current study. A higher impact of PsA-related comorbidities on mortality among women compared with men could, however, be hypothesised, and also receives some support from the observation that the percental differences in deaths due to CVD and infections between patients and comparator-subjects were marginally higher for women than men (table 3). The finding that the mortality risk in relation to age-matched and sex-matched comparator-subjects increases with longer duration since diagnosis is compatible with negative effects of long-term systemic inflammation, and may also reflect the accumulation of PsA-related comorbidities over time.
Of note, while we do observe an increased all-cause mortality in the overall PsA population, the risk-increase of around 10% is lower than that previously reported for RA (estimated excess risk 24–126%) or AS (38–64%).15–20 This may also partly explain the conflicting results of prior PsA studies, some of which may have been underpowered to detect a risk-increase of this size. Interestingly, prior studies have found a more clearly elevated mortality risk in PsO than in PsA.27 36 While this could be due to different effects of skin and joint inflammation, it may also be hypothesised that one mechanism underlying such results could be that patients with mild PsO more often than PsA may not seek medical care at all, or are managed exclusively in primary care, rendering them not to be included in mortality assessments. Anyhow, in a recent meta-analysis, the all-cause mortality in PsO (of any severity) was increased in the same general range as that observed for PsA in the present study (pooled relative risk 1.21 (95% CI: 1.14 to 1.28)), whereas it was higher in severe PsO.37
To estimate cause-specific mortality was beyond the aims of the present study. However, apart from the minor sex-differences alluded to above, the cause of death distributions were overall similar between PsA cases and comparator-subjects. In accordance with a number of previous publications,18 29 33 35 36 deaths due to CVD and malignancy were the leading causes in both groups.
Within our PsA population, disease severity, as reflected by previous joint surgery, was a significant predictor of all-cause mortality. Of particular interest, prior hip and/or knee replacement surgery was a stronger mortality predictor in PsA than in comparator-subjects. Prior studies regarding the predictive roles of disease activity and severity on mortality in PsA are limited. In two earlier studies, higher disease activity and elevated acute phase reactants were, however, associated with an increased risk of death in PsA.28 32 General comorbidities were strong predictors of mortality in both PsA and comparator-subjects, whereas extra-musculoskeletal manifestations (ie, IBD, uveitis) did not predict increased mortality in PsA, despite IBD being related to mortality in the population. Our results also indicate that the relative contribution of some conditions, in particular anxiety/depression, to mortality may be greater in the general population than in patients with PsA, where disease-specific factors also play a role. Finally, lower socioeconomic status, approximated by shorter education, was a significant non-differential predictor of mortality among PsA cases and comparator-subjects, in accordance with prior assessments in both PsA and the general population.32 35 47
Strengths and limitations
The large size (the largest to date on this topic) and population-based approach of our study, including patients with PsA with variable disease severity, is expected to provide estimates close to the true MR. The register-based methodology allowed nationwide identification of PsA cases and comparator-subjects from the general population in a uniform and systematic manner. This enabled direct comparisons with internal comparator-subjects, which has previously been shown to yield better mortality approximations than external comparisons (SMRs).48
PsA cases managed exclusively in primary care, as well as a minority subset of cases managed only by private caregivers, are not captured by the NPR and thus not included in the current study. The proportion of individuals with only primary care health contacts for PsA has been estimated at 8.5% and 26.7%, respectively, in two assessments from southern Sweden prior to 2010.38 49 In the first of these studies, however, only 18–24% of the PsA cases with a diagnosis deriving exclusively from primary care were found to fulfil established PsA classification criteria.38 The proportion of PsA cases exclusively followed in private specialised care units that do not report to the NPR (which most nowadays do) is expected to differ regionally, depending on the availability of private caregivers. Patients followed at such units might, however, occasionally also consult public rheumatology departments. Considering that both of these groups of patients may have a milder disease than those included in our study, the observed mortality risk could be somewhat overestimated, although the exact size of such overestimation is unknown.
Furthermore, the validity of the PsA diagnoses in the NPR may be a potential limitation. However, the PsA case definition used for the present assessment has shown high validity, with a positive predictive value for the fulfilment of established PsA classification criteria of 86%.46 Misclassification of PsA diagnoses in the NPR is thus unlikely to have had a substantial impact on our mortality estimates, which is further supported by the similar results in the sensitivity analysis in which 20% of the PsA cases were randomly replaced by one of their own matched comparator-subjects. Misclassification of the main outcome is not a major concern because of virtually complete ascertainment, but misclassification of the cause of death is likely to be present despite the reliable data deriving from the Cause of Death Register. However, this misclassification is possibly non-differential for the PsA cases and comparator-subjects and unlikely to have significantly flawed our results.
Finally, the nationwide register sources used for the current study unfortunately do not provide sufficient coverage regarding lifestyle factors, disease characteristics and clinical variables that would allow for adjustment or stratification for important variables such as smoking, other risk factors for CVD not captured by ICD-codes, disease severity or PsA phenotype. Nor do we know the time of symptom onset, and thus used time since PsA diagnosis as surrogate marker for disease duration. In light of the clear risks of confounding by indication in relation to comorbidities, as well as difficulties to distinguish impact of treatments from that of disease activity, attempting to assess potential relationships between anti-rheumatic treatment exposures (non-steroidal anti-inflammatory drugs, glucocorticosteroids, DMARDs) and mortality in PsA would require a dedicated study in its own right, and was thus beyond the scope of the present manuscript.
Conclusions
In conclusion, in this large, population-based study from Sweden, the mortality risk in PsA was estimated at about 10% higher than in the general population, with increased risks mainly in women and patients with longer disease duration (time since PsA diagnosis), and emanating from an excess comorbidity burden. The cause of death distribution in PsA was similar to that in the general population. However, further studies are warranted to disentangle the effects of disease activity and medication on mortality risk.
Data availability statement
Data may be obtained from a third party and are not publicly available. The study was conducted using de-identified participant data from various national Swedish administrative and healthcare registers. For further information the corresponding author JKW (johan.81.karlsson@gmail.com) may be contacted.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval was granted by the Regional Ethics Committee in Stockholm, Sweden (Dnr. 2015/1844-31/2). Consent from individual patients or comparator-subjects was not required by the ethical approval.
Acknowledgments
A special thanks to our patient representative Britt Nilsson for her valuable input. We would like to thank Dr Gerd-Marie Alenius (Umeå University) for her contribution to the planning of the study and discussion of the study results. The initial findings of the work presented in this manuscript have been presented as an oral presentation (OP0218) at the European Alliance of Associations for Rheumatology (EULAR) congress 2021 (virtual) (http://dx.doi.org/10.1136/annrheumdis-2021-eular.104).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Josef S Smolen
Twitter @ValgerdurRos
Contributors SE, DDG, LTHJ, JA and JKW contributed to the conception and design of the study. JKW performed the statistical analyses. All authors contributed to acquisition and interpretation of data. SE and JKW drafted the manuscript. All authors critically reviewed the manuscript for important intellectual content. All authors approved the final manuscript to be published and agree to be accountable for all aspects of the work. JKW is the guarantor for this manuscript.
Funding This study was supported by AbbVie, Amgen, Eli Lilly, Novartis and Pfizer. The sponsors were allowed to comment on the study protocol and were provided with a report of the results, but had no influence on the study design, data collection, data analysis, data interpretation, writing of the report or decision to submit the manuscript. This study was further supported by unrestricted grants from Psoriasisförbundet, Gösta A Karlssons 60-årsfond, Reumatikerförbundet and Skåne University Hospital.
Competing interests SE: Grant/research support from AbbVie, Amgen, Eli Lilly, Novartis and Pfizer (as detailed under Funding statement); Consulting fees from Amgen, Janssen, Novartis and UCB Pharma. DDG: None declared. EK: Speaker’s bureau fees from Amgen, Janssen, Pfizer and UCB Pharma. VS: Speaker’s bureau fees from AbbVie, AstraZeneca and Novartis; Advisory board participation for AbbVie, Galapagos, Janssen, Novartis, Sanofi and UCB Pharma. SW: None declared. UL: None declared. CT: Grant/research support from BMS; Speaker’s bureau fees from AbbVie, BMS, Nordic Drugs, Pfizer and Roche; Advisory board participation for Roche. LTHJ: Speaker’s bureau fees from AbbVie, Janssen and Novartis; Advisory board participation for AbbVie, Eli Lilly, Janssen, Novartis and Pfizer. JA: Grant/research support for the Swedish biologics register ARTIS from AbbVie, BMS, Eli Lilly, Galapagos, Merck, Pfizer, Roche, Samsung Bioepis, Sanofi and UCB Pharma. JKW: Grant/research support from AbbVie, Amgen, Eli Lilly, Novartis and Pfizer (as detailed under Funding statement); Speaker′s bureau fees from AbbVie and Amgen.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.