Article Text

Abstract
Objectives Treatment targets in systemic lupus erythematosus (SLE) have been validated in unselected—in terms of severity—cohorts, which limits their generalisability. We assessed remission (Definition of Remission in SLE (DORIS)) and Lupus Low Disease Activity State (LLDAS) in a historical cohort of 348 patients with active moderate-to-severe disease and median follow-up of 5 years.
Methods Active SLE was defined as Physician Global Assessment ≥1.5 and/or SLE Disease Activity Index 2000 ≥6, requiring therapy intensification. DORIS/LLDAS, organ damage, flares and adverse events were monitored. Shared frailty survival, generalised linear models and K-means clustering were applied.
Results Sustained DORIS and LLDAS for ≥6 months occurred in 41.1% and 80.4%, respectively, and resulted in reduced damage accrual (HR: 0.58; 95% CI 0.36 to 0.93 and 0.61; 0.43 to 0.86) and severe flares (HR: 0.14; 0.08 to 0.27 and 0.19; 0.13 to 0.27). LLDAS without DORIS was also protective (HR: 0.65; 0.43 to 0.98 for damage, 0.49; 0.36 to 0.67 for flares). Models fitting increasing duration of targets showed that DORIS ≥50% and LLDAS ≥60% of time, or alternatively, ≥24 and ≥36 months, achieved optimal balance between feasibility (20.2–41.7%) and specificity (73.3–86.1%) for damage-free outcome. These targets were linked to reduced serious adverse events (risk ratio (RR): 0.56–0.71), hospitalisation (RR: 0.70) and mortality (RR: 0.06–0.13). Patients with predominant arthritis and mucocutaneous disease experienced reduced DORIS/LLDAS, compared with counterparts with major organ involvement. Conventional drugs were more frequently used in the former group, whereas potent immunosuppressive/biological agents in the latter.
Conclusions In moderate-to-severe SLE, sustained DORIS/LLDAS for at least 6 months is sufficient, while attainment for at least 24 months ensures higher specificity for damage-free progression, thus facilitating treat-to-target strategies and clinical trials. Arthritis and skin disease represent unmet therapeutic needs that could benefit from novel biologics.
- Lupus Erythematosus, Systemic
- Therapeutics
- Outcome Assessment, Health Care
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplemental information. Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Remission (Definition of Remission in SLE (DORIS)) and Lupus Low Disease Activity State (LLDAS) have been introduced in systemic lupus erythematosus (SLE), yet their feasibility and validity have not been evaluated in patients with moderate or high disease activity and severity.
WHAT THIS STUDY ADDS
In active moderate/severe SLE, DORIS and LLDAS are pragmatic targets that reduce organ damage accrual and severe flares. LLDAS, irrespective of achievement of DORIS, is also protective.
At least 6 months of sustained DORIS/LLDAS is sufficient for protection; at the individual-level, prolonged achievement of these targets (at least 24 months) has high specificity (>80%) for damage-free prognosis and protects against multiple other adverse outcomes, suggesting they might be useful for treat-to-target strategies and clinical trial design.
Lupus arthritis and mucocutaneous disease predominantly managed with conventional agents exhibit increased propensity for flaring and reduced achievement of the treatment targets.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Validation of DORIS and LLDAS in patients with moderate/severe SLE supports the wider adoption of these targets in routine practice. Skin and joint diseases represent unmet therapeutic needs in SLE, urging for the introduction of novel targeted interventions.
Introduction
The treat-to-target paradigm has been successfully applied to many chronic conditions, including inflammatory arthritides.1 In systemic lupus erythematosus (SLE), two widely accepted treatment targets have been proposed, namely the Definition of Remission in SLE (DORIS)2–4 and the Lupus Low Disease Activity State (LLDAS).5 Observational studies have shown that patients who achieve these targets exhibit reduced rates of organ damage accrual and flares.6–11 Attainment of either DORIS12 or LLDAS13–15 has been associated with improvements in health-related quality of life, confirmed also in the setting of randomised controlled trials (RCTs).16 Based on this evidence, the European Alliance of Associations for Rheumatology (EULAR) has recommended that SLE treatment should be tailored to reach the aforementioned targets.17
A crucial issue pertains to the feasibility and generalisability of the treatment targets across different clinical scenarios. With a few exceptions,9 previous studies have evaluated the LLDAS and DORIS definitions in unselected SLE cohorts with no explicit disease activity entry criteria. This might have skewed the results as patients with milder disease are more likely to attain the targets18 and display overall better long-term outcomes. Indeed, in the study by Golder et al,11 less than 30% of patients had SLE Disease Activity Index 2000 (SLEDAI-2K) ≥6 at inclusion; in this group, LLDAS occurred less frequently as compared with counterparts with SLEDAI-2K <6 (23.6% vs 58.7%, respectively). This trend is also reflective on the low prevalence of LLDAS19–21 and DORIS22 at week 52 in lupus RCTs, which typically enrol patients with moderate or high disease activity. A closely related matter is that patients with higher degrees of activity/severity tend to receive more glucocorticoids,23 especially at the early phases of treatment, which could potentially dampen the damage-protective effects of low disease activity or remission states attained later during the disease course.
To address these issues, we designed a study to include patients with SLE with prespecified criteria for moderately-to-severely active disease, who were followed with multiple consecutive visits over a median of 5 years. In addition to analysing the attainment of remission (DORIS) and low disease activity (LLDAS), overlapping or not with remission, at each visit and cumulatively over time, we deployed multiple methodologies to ascertain their effect against damage accrual and severe flares. By comparing models of different stringency, we introduced target exposure thresholds of high specificity for favourable prognosis and validated them against the risk of secondary relevant outcomes such as adverse events, hospitalisation and death. Finally, by dissecting the clinical heterogeneity of our cohort and analysing the treatment patterns, we identified endotypes associated with lower attainment of the targets, thus unravelling unmet therapeutic needs in SLE.
Patients and methods
Study design, inclusion criteria and participants
This is a retrospective cohort study of patients with SLE aged ≥16 years who fulfilled the 2012 Systemic Lupus International Collaborating Clinics (SLICC)24 and/or 2019 EULAR/American College of Rheumatology (ACR) classification criteria,25 and were followed during January 2008–June 2018 in two centres with dedicated lupus clinics and registries (Heraklion, Ferrara). Patients were included if they had SLEDAI-2K ≥626 and/or Physician Global Assessment (PGA) ≥1.5,27 necessitating increase or intensification of treatment as follows28: (1) initiating glucocorticoids either oral at a dose of ≥20 mg/day (prednisone equivalent) and/or intravenous pulse methylprednisolone; (2) increasing (at least doubling) the dosage of glucocorticoids; (3) initiating immunosuppressive (including calcineurin inhibitors) or biological (including intravenous immunoglobulin) agents. The requirement for therapy intensification was introduced to ascertain medium/high disease activity. Patients with coexisting systemic autoimmune/inflammatory disorders were excluded. For each patient, the inclusion date was identified by screening the medical charts, starting from the earliest available visit and forward in time until the first fulfilment of the entry activity criterion. Baseline and follow-up data were collected from the inclusion and all succeeding visits in a prospective manner. The minimum required visit frequency was every 6 months during the first year since inclusion and then every 12 months, although most patients had more frequent visits (approximately every 4–6 months) at the physician’s discretion. Out of 887 patients screened, 284 were excluded for not meeting the inclusion criteria and another 245 due to diagnosis prior to 2008.
Clinical assessment and variables collection
The two centres have been already collaborating in clinical projects and use homogenised protocols for SLE assessment with structured data collection forms.29 At inclusion, demographics, the date of diagnosis and fulfilment of the classification criteria, smoking status (never, former, current smoker), major comorbidities and previous treatments were captured. At each visit, the following data were monitored: ongoing treatments and their dosage; SLE activity (SLEDAI-2K,26 PGA on a scale of 0–327); disease flares (Safety of Estrogens in Lupus Erythematosus National Assessment (SELENA)-SLEDAI Flare Index27 modified to include mycophenolate, belimumab and rituximab under the definition of severe flare); irreversible organ damage (SLICC/ACR Damage Index (SDI)30); comorbidities and adverse events including death (Common Terminology Criteria for Adverse Events (CTCAE); https://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm) (see online supplemental methods for more details). In accordance to the standard practice of the clinical centres, PGA was scored before immunological tests were available. Laboratory results obtained within 30 days of each visit were considered for completing the SLEDAI-2K. Attainment of low disease activity and remission was determined at each visit according to the published LLDAS5 and DORIS2 definitions (online supplemental table S1). Following pseudo-anonymisation, data were entered into a secure electronic registry.
Supplemental material
Supplemental material
Study outcomes and sample size estimation
The two primary outcomes were organ damage accrual (any increase in SDI) and severe flares. Secondary outcomes comprised adverse events (of any severity), serious adverse events (non-fatal and those requiring hospitalisation) and death. We tested the association between each aforementioned outcome with the LLDAS and DORIS states examined either as attainment at any single visit or cumulative observed time in each state. Details on sample size estimated are provided in the online supplemental methods.
Statistical analysis
The multiple-failures Cox-proportional hazards model was employed to determine the relationship between LLDAS or DORIS attainment at each visit and within each patient, with the risk of subsequent damage accrual (≥1-point increase in SDI) and severe flares. To account for the possibility that some patients may be more failure prone than others, we introduced a shared frailty option in the hazard models. Patient survival time data were used to estimate incidence rates for the outcomes. We calculated for each patient (1) the percentage of observation time in each target by summing of all intervals in the target divided by the total observation period and multiplied by 100,11 and (2) the total consecutive months spent in each target (applied to 92.8% of the cohort with ≥24-month follow-up). Generalised linear models were used to test the effect of increasing thresholds of exposure time in LLDAS or DORIS on the risk of damage accrual and severe flares. We chose specific time thresholds of the targets in order to classify patients and produce corresponding multiple-failures hazard models. In an ancillary approach, we also modelled standard Cox regression on the time-to-first incidence of the primary outcomes.
K-means was used to cluster patients according to the proportion of time exhibiting activity from each SLEDAI-2K item. Due to the low frequency of certain manifestations, the items from the neurological, renal and serositis domains were grouped together. The optimal number of clusters was defined by the Silhouette method. For each cluster, we computed the average proportion of follow-up time with activity in each SLEDAI-2K item/domain, relative to the entire study population average, followed by calculation of relative fold changes across the clusters. The corresponding heatmap was generated with pheatmap (V.1.0.12). Statistical analysis was performed using STATA V.18.0 using the stpm2 31 and bsurvci 32 commands.
Results
DORIS and LLDAS are feasible targets in active moderate-to-severe SLE
We studied 348 patients (92.8% females) monitored over a median (IQR) period of 60 (27) months with 10 (4) visits per patient and 6.0 (3.0) months between-visit interval, thus totalling 18 777 person-months (table 1). At inclusion, the median (IQR) PGA, SLEDAI-2K and clinical SLEDAI-2K (excluding serology) were 2.0 (0.5), 8 (4) and 6 (4), respectively, thus indicative of moderate-to-high activity/severity. Most frequently involved domains at baseline were the musculoskeletal (69.3%) and mucocutaneous (62.4%), followed by the haematological (17.5%), renal (16.7%), serositis (9.2%) and neurological (5.5%) (online supplemental table S2).
Demographic and clinical characteristics of patients with SLE at inclusion visit and during follow-up
During follow-up, DORIS and LLDAS were achieved at least once by 215 (61.8%) and 323 (92.8%) patients, respectively (table 1). The median (IQR) time to first occurrence of DORIS was 15 (20) months, and the respective estimate for LLDAS was 9 (9) months. A total of 97 (27.9%) and 193 (55.5%) patients spent ≥24 months in DORIS and LLDAS, respectively ().
These results indicate that both targets are attainable in patients with active moderate-to-severe SLE, with LLDAS showing higher feasibility over DORIS. Indeed, out of 1577 LLDAS visits, 771 (48.9%) met the DORIS definition (LLDAS+/DORIS+) while the remaining 806 (51.1%) did not (LLDAS+/DORIS–), thus suggesting that LLDAS overlaps partially with DORIS and a proportion of patients may fall into a distinct state of low or minimal—but not zero—disease activity.
Treatment targets are protective against damage accrual and severe flares in patients with moderate-to-severe SLE
Patients with higher SLE activity are typically managed with more glucocorticoids, as highlighted in our cohort (table 1), and they tend to develop more frequently organ damage and flares.23 Therefore, we examined whether the existing targets are protective in moderate-to-severe disease. In a visit-by-visit analysis, DORIS and LLDAS were both associated with reduced risk of new organ damage (HR; 95% CI 0.64; 0.42 to 0.97 and 0.63; 0.46 to 0.89, respectively) and severe flares (HRs 0.34; 0.22 to 0.51 and 0.39; 0.29 to 0.51, respectively) at subsequent visit (table 2).
Attainment of DORIS and LLDAS associated with reduced accrual of damage and severe flares in patients with active moderate-to-severe SLE (visit-by-visit analysis)
LLDAS+/DORIS– visits were also protective (HR 0.65; 0.43 to 0.98 for damage, and 0.49; 0.36 to 0.67 for flares, respectively). Compared with DORIS, LLDAS+/DORIS– visits had comparable risk of subsequent new damage (HR 1.12; 0.68 to 1.86) but increased hazard for severe flares (HR 1.78; 1.11 to 2.83). This difference was driven primarily by the residual disease activity in LLDAS+/DORIS– state (online supplemental table S3).
Using the median time to achievement of each target as a threshold, we found that both early and late achievement of DORIS and LLDAS were related to reduced future organ damage and severe flares (table 2). With regard to target duration, sustained achievement of either target for at least 6 months was sufficient for a significant risk reduction in the adverse outcomes, with longer attainment periods showing more pronounced effects. In agreement with the Cox regression, increasing percentage of time in DORIS and LLDAS correlated with decreasing risk of damage and severe flares (online supplemental table S4). Notably, the percentage of time in LLDAS+/DORIS– exhibited an additional protective effect.
To address the impact of different levels of target achievement, we created non-mutually exclusive patient groups according to increasing thresholds (% of time) in each target, followed by generalised linear models for the primary study outcomes. We noted a gradual decrease in the relative risk (RR) (ie, greater risk reduction) for organ damage and severe flares with increasing thresholds (≥30–≥70%) of cumulative time in DORIS and LLDAS (online supplemental figure S5 and online supplemental table S5). These results support the damage-protective and flare-protective effects of sustained DORIS and LLDAS, the latter irrespective of complete clinical remission (DORIS), in patients with moderate/severe lupus. In agreement with the visit-by-visit analysis, patients who experienced LLDAS+/DORIS– ≥50% of time had increased risk of severe flares (but not organ damage) compared with those with DORIS ≥50% of time (online supplemental table S6).
Supplemental material
Definition of time thresholds of DORIS and LLDAS attainment with optimal balance between feasibility and protection against adverse outcomes in moderate-to-severe SLE
While RR estimates demonstrate the strength of association between target achievement and outcomes, they are not useful for individual-level classification which may be relevant to clinical decision-making and treat-to-target implementation. To this end, we used the patient groups shown in online supplemental figure S1, in order to determine the frequency of each exposure cut-off in DORIS and LLDAS, as well as its specificity for damage-free progression (online supplemental table S7). Taking into account these parameters as well as the goodness-of-fit measures of the corresponding statistical models (Online supplemental figure S1A,B), we found that DORIS ≥50% and LLDAS ≥60% of cumulative time had the best trade-off between feasibility, model stability and protection against organ damage (specificity 85.2% and 73.3%, respectively) (table 3).
Durable attainment of treatment targets based on time exposure thresholds with high specificity for organ damage-free and severe flare-free progression in patients with active moderate-to-severe SLE
To obtain thresholds expressed in actual time units, we carried out a similar analysis with increasing cut-offs of consecutive months in each target spanning the 5–95 percentile range within the DORIS ≥50% and LLDAS ≥60% groups (10.5–58.0 and 13.5–58.0 months, respectively) (online supplemental table S8). DORIS ≥24 months and LLDAS ≥36 months showed optimum performance with specificity 86.1% and 81.2%, respectively, for damage-free progression (table 3).
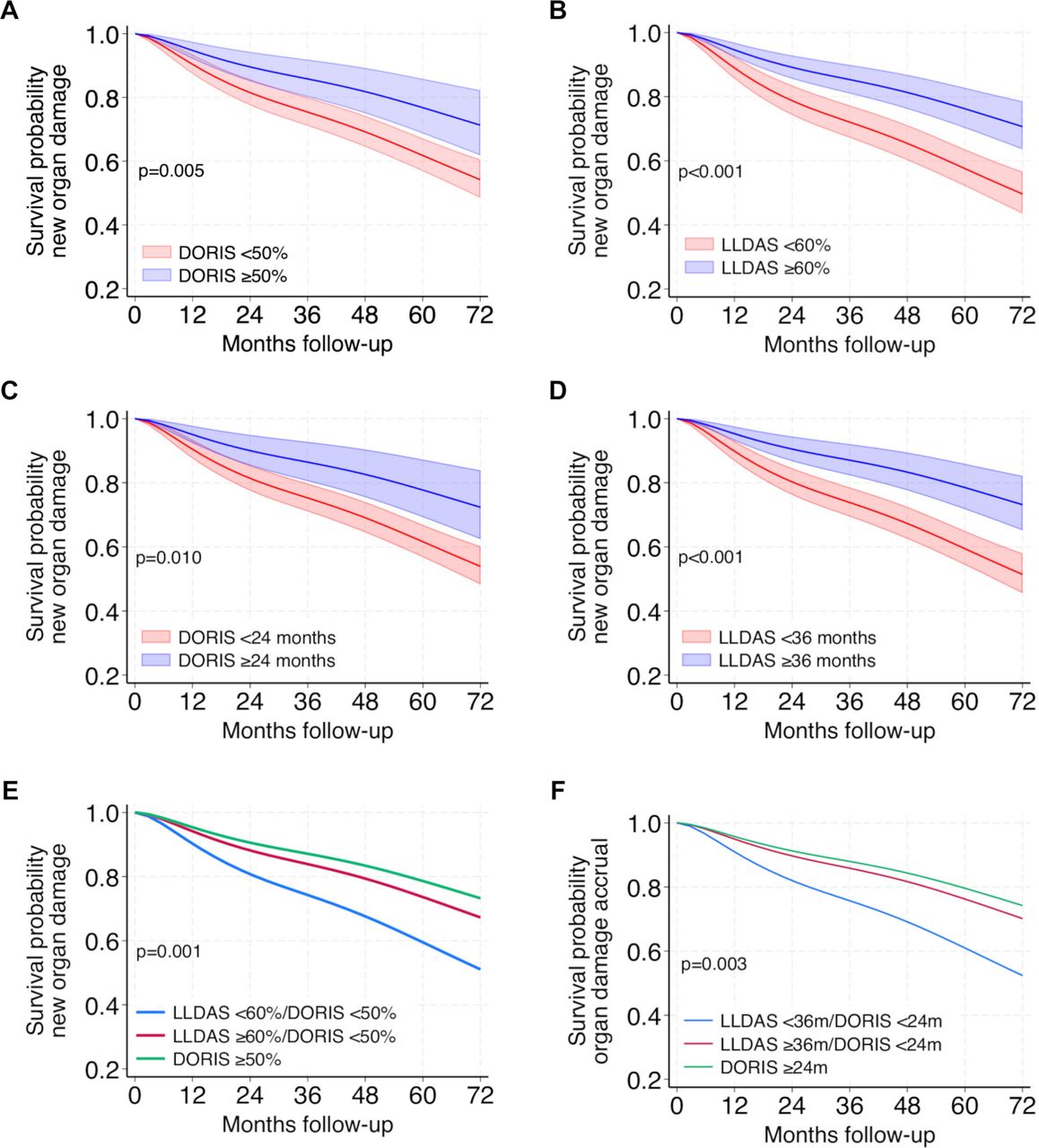
To further ascertain the prognostic value of these goals, we grouped our patients according to whether or not they achieved the aforementioned cut-offs, followed by multiple-failures Cox regression. Both DORIS ≥50%/≥24 months and LLDAS ≥60%/≥36 months were associated with significantly reduced hazards for new organ damage (figure 1A–D) and severe flares (online supplemental figure S3A–D) (see the corresponding figure legends for the exact estimates) and similar results were found in the time-to-first event analysis (online supplemental figure S4). Patients who attained LLDAS ≥60% without DORIS ≥50% or LLDAS ≥36 months without DORIS ≥24 months were also protected against adverse outcomes (figure 1E,F and online supplemental figure S3E,F).

Attainment of treatment targets above specific exposure thresholds results in significant reduction of organ damage accrual. (A,B) Survival plot of new organ damage-free time according to achievement of (A) DORIS ≥50% of observation time or not (HR 0.51; 95% CI 0.31 to 0.84, multiple-failures Cox-proportional hazards), and (B) LLDAS ≥60% of time or not (HR 0.47; 0.32 to 0.69). Banded areas represent 95% CI. (C,D) Survival plot of new organ damage-free time according to sustained attainment of (C) DORIS ≥24 months or not (HR 0.49; 0.29 to 0.84, multiple-failures Cox-proportional hazards) and (D) LLDAS ≥36 months or not (HR 0.43; 0.28 to 0.68). Banded areas represent 95% CI. (E) The same plot as above according to accomplishment of DORIS ≥50% of time (with or without LLDAS ≥60% of time), LLDAS ≥60%/DORIS <50% and LLDAS <60%/DORIS <50%. Using the latter condition as reference, LLDAS ≥60%/DORIS <50% had reduced hazard for organ damage accrual (HR 0.60; 0.38 to 0.95, p=0.030). (F) The same plot as above according to sustained attainment of DORIS ≥24 months (with or without LLDAS ≥36 months), LLDAS ≥36 months/DORIS <24 months and LLDAS <36 months. Using the latter condition as reference, LLDAS ≥36 months/DORIS <24 months had reduced hazard for organ damage accrual (HR 0.54; 0.30 to 0.97, p=0.038). DORIS, Definition of Remission in SLE; LLDAS, Lupus Low Disease Activity State.
Achievement of time-defined treatment goals (DORIS ≥50%/24 months, LLDAS ≥60%/36 months) is associated with reduced incidence of adverse events, hospitalisation and mortality in patients with SLE
In individuals with SLE, the interplay of disease activity/inflammation and glucocorticoid intake drives the development of comorbidities and death.33–40 We tested the above-defined thresholds of DORIS and LLDAS against the accrual of adverse events classified by the CTCAE system, which captures infections, cardiovascular events, disorders from any organs, laboratory abnormalities, etc. Patients who spent DORIS ≥50% in time experienced an average of 2.14 events per 100 patient-months as compared with their counterparts with DORIS <50% in time who had 5.54 events per 100 patient-months (incidence rate ratio (IRR) 0.77;95% CI 0.68 to 0.87) (table 4). The respective figures for patients in LLDAS ≥60% vs <60% were 3.53 and 5.63 events per 100 patient-months (IRR 0.88; 0.82 to 0.94). We performed further analysis according to the severity of events (physician ascertained) and healthcare utilisation. For both serious events (composite including the CTCAE grading serious, life-threatening or lethal) and events leading to hospitalisation, sustained DORIS ≥50% and LLDAS ≥60% resulted in significant risk reductions (IRRs 0.56–0.71) irrespective of the effect of age, gender and baseline disease activity. Finally, despite the low number of deaths (n=6) during follow-up, DORIS ≥50% and LLDAS ≥60% were associated with reduced mortality. Similar protective trends were noted for patients who achieved DORIS ≥24 months and LLDAS ≥36 months compared with those who did not meet these thresholds (online supplemental table S9).
Attainment of DORIS ≥50% and LLDAS ≥60% of time is linked to reduced incidence of adverse events including hospitalisation and mortality in patients with SLE
The type of organ involvement correlates with the attainment of treatment targets in moderate-to-severe SLE
Despite similar starting levels of SLE activity/severity, patients in our study showed variable achievement of the treatment targets. Baseline SLEDAI-2K and PGA were not significant determinants of either target (data not shown). This prompted us to explore whether distinct clinical endotypes could have been associated with differences in experiencing DORIS and LLDAS. By performing unsupervised clustering in the longitudinal data, three major subgroups were identified according to the cumulative time of activity from various organs/domains (online supplemental figure S5 and figure 2A). Cluster 1 (25.0% of the cohort) had increased prevalence of serositis, vasculitis, renal and serological domains; cluster 2 (39.9%) had increased prevalence of serositis, thrombocytopenia and neurological disease; and cluster 3 (35.1%) was characterised by predominant mucocutaneous and joint disease. Baseline disease activity/severity was comparable between the three groups (median (IQR) clinical SLEDAI-2K: 6 (4), 6 (4), 6 (2) and PGA: 2.0 (0.5), 2.0 (0.5), 1.5 (0.5), in clusters 1–3, respectively). Cluster 2 patients displayed the highest achievement of targets (median time in DORIS and LLDAS: 37.8% and 68.5%, respectively), followed by cluster 1 patients (23.2% and 55.6%). By contrast, the lowest target attainment was observed in cluster 3 (0.0% and 29.7%) (figure 2B,C). These relative differences persisted after excluding the mucocutaneous and arthritis items from the DORIS/LLDAS definitions (online supplemental figure S6). Although the three clusters had comparable accrual and pattern of new organ damage, cluster 3 was linked to significantly higher rate of flares compared with clusters 1–2 (online supplemental tables S10 and S11).

{kind=link}
{kind=link}
Clinically defined SLE patient clusters correspond to differential attainment of the DORIS and LLDAS treatment targets. (A) K-means clustering was used to group patients according to the proportion of follow-up time exhibiting activity in each one of the items/domains included in the SLEDAI-2K. Clusters 1 (n=87, 25.0% of the study cohort), 2 (n=139, 39.9%) and 3 (n=122, 35.1%) were identified. Heatmap illustrating the fold changes of the proportion of time with actively involved SLEDAI-2K items, across the patients’ clusters. Z-score transformation of the fold change values was applied, ranging from −1 (dark blue) to +1 (dark red) as shown in the legend on top right. ‘Serositis’ includes ‘pericarditis’ and ‘pleuritis’; ‘renal features’ include ‘urinary casts’, ‘haematuria’, ‘proteinuria’ and ‘pyuria’; and ‘neurological features’ include ‘seizure’, ‘psychosis’, ‘organic brain syndrome’, ‘visual disturbances’, ‘cranial nerve disorder’ and ‘lupus headache’. (B) Dot plots demonstrating the attainment (% of cumulative time) of DORIS and LLDAS by each patient across the three clusters. The black dot with blue error bars represents the median (IQR) attainment in each cluster. Comparisons between the clusters were performed with the Kruskal-Wallis non-parametric test followed by Dunn’s test for multiple comparisons. *P<0.05; ***P<0.001; ****p<0.0001. (C) Stacked bar plots illustrating the proportion of patients within each cluster who met the target thresholds DORIS ≥50% (with or without LLDAS ≥60%), LLDAS ≥60%/DORIS <50% and LLDAS <60%/DORIS <50%. DORIS, Definition of Remission in SLE; LLDAS, Lupus Low Disease Activity State; SLE, systemic lupus erythematosus; SLEDAI-2K, SLE Disease Activity Index 2000.
To dive in further into these results, we analysed treatment patterns according to organ involvement. Mucocutaneous manifestations and arthritis, over-represented in cluster 3, were most frequently treated with conventional agents such as methotrexate and azathioprine. Conversely, manifestations prevailing in clusters 2 and 3 were often managed with more potent immunosuppressants (mycophenolate, cyclophosphamide) or biological agents (belimumab, rituximab) (online supplemental table S12). Although these relationships do not imply causality and may be subject to unmeasured bias; nonetheless, they are suggestive of insufficient control of lupus skin and joint disease resulting in increased propensity for flaring and decreased attainment of the therapeutic goals.
Discussion
Here, we show that in active moderate/severe SLE (median SLEDAI-2K: 8, PGA: 2.0), both remission (DORIS) and low disease activity (LLDAS) are pragmatic targets that protect against organ damage and severe flares. We provide evidence that LLDAS exclusive of remission is also protective against these outcomes. In addition, exposure-defined thresholds of the targets are introduced as putative therapeutic goals that might assist the treat-to-target implementation and trial design. Importantly, these target thresholds are validated for their beneficial effects on damage, flares and other important patient outcomes such as adverse events, hospitalisation and mortality. Finally, we define major disease endotypes and demonstrate that patients with predominant arthritis and skin/mucosal disease have the lowest achievement of targets, suggesting they could benefit from the introduction of novel target therapies in SLE. Our findings are in line with the EULAR recommendations17 proposing remission and low disease activity as therapeutic goals in SLE, and provide support for the wider adoption of these targets in clinical care.
We focused on moderate or severe SLE requiring therapy intensification as it remains elusive whether the existing definitions of remission/LLDAS are feasible and effective in this disease population, which has been under-represented in previous studies. These patients typically commence with higher disease activity and are exposed to more glucocorticoids, thus making it more arduous to reach the recommended targets11 18 while also increasing the risk of damage.23 DORIS and LLDAS were reached by the majority of patients (61.8% and 92.8%) on at least one visit, and by a sizeable proportion for at least 6 consecutive months (41.1% and 80.4%). Our results align with those of Kikuchi et al 41 who evaluated 79 patients with active/severe SLE (applying different criteria) and found that 89.9% of them experienced LLDAS. Importantly, we found a significant protective effect of DORIS and LLDAS against accrual of organ damage and severe flares, which corroborates their validity and generalisability in moderate/severe SLE.
LLDAS was intersected with DORIS in about 50% of visits, which is lower than the LLDAS/DORIS overlap shown in previous studies,7 10 18 42 possibly due to differences in patient characteristics and duration of follow-up. To this end, it remains uncertain whether LLDAS exerts an additional protective effect over remission.7 10 42 In our analysis, LLDAS+/DORIS– visits had significantly reduced hazard for subsequent development of organ damage and severe flares, which was confirmed by demonstrating an independent effect of the duration of this state. This result is plausible considering the linear-type association of SLEDAI43 and glucocorticoid intake42 44 with the risk of adverse outcomes such as organ damage. From a clinical standpoint, LLDAS+/DORIS– and LLDAS+/DORIS+ may represent a continuum of states displaying a gradient of association with favourable patient prognosis. A similar concept has been described in rheumatoid arthritis, where Disease Activity Score-28-defined remission and low disease activity may be protective against clinical and radiological outcomes45 46 with remission showing more consistent associations.47 48 Our findings support the recommendations that remission is the preferred goal with low disease activity representing a valid alternative.17
The protective effect of target attainment against organ damage and severe flares was prominent in patients with sustained DORIS and LLDAS for at least 6 months. Studies in different settings and cohorts have suggested that the shortest length of targets associated with a decrease in damage progression may range from as low as 3 months for LLDAS11 to at least 2 consecutive years for remission and LLDAS.7 42 49 These results underscore the importance of prolonged disease stabilisation with appropriate treatment modifications, if required, to ensure optimal long-term outcomes in SLE.
In the same context, increasing thresholds of observed time in targets correlated positively with a protective effect but at the cost of decreasing attainability. Previous studies have focused on the 50% cut-off in remission9 10 or LLDAS5 8 11 18 41 to classify patients at lower versus higher risk of damage and flares, although lower thresholds have also been suggested.6 11 Following an unbiased methodology, we found that DORIS ≥50% and LLDAS ≥60% of the cumulative time (or ≥24 and ≥36 consecutive months, respectively) had the best combination of prevalence/sensitivity and specificity for damage-free progression. Pending further confirmation, the sufficiently high specificity of these cut-offs (73.3–86.1%) suggests they could assist individualised risk assessment and treat-to-target implementation. It might also be interesting to explore the performance of the time proportion thresholds in the context of SLE trials, in view of evidence suggesting that DORIS and LLDAS might serve as outcome measures in discriminating active drug versus placebo.19
We verified the impact of exposure-defined DORIS and LLDAS goals by documenting their association with lower incidence of adverse events, related hospitalisation and death. This corroborates previous reports in SLE showing that prolonged attainment of either target may reduce mortality.8 50 The relationship between DORIS or LLDAS with the incidence risk of adverse events and/or hospitalisation is novel and reminisces similar protective effects of remission and low disease activity in rheumatoid arthritis.46 These results add to the spectrum of beneficial effects associated with the accomplishment of remission and low disease activity in SLE, thus validating further their use in clinical care.
Our observation of lower DORIS/LLDAS rates (accompanied by increased flares) in patients with predominant mucocutaneous and joint disease agrees with previous studies in white patients18 42 and merits further discussion. Although these particular manifestations might be inherently difficult to treat, they were more frequently managed with methotrexate, azathioprine and, to a lesser extent, leflunomide, belimumab or rituximab. It should be emphasised that these relationships do not prove causality and some of the drug choices might have been directed by physicians’ and patients’ preferences or intolerance issues. The lower frequency of DORIS/LLDAS might also relate to the SLEDAI instrument, which requires the complete resolution of arthritis, rash, etc in order for the corresponding items to receive 0 score. Nonetheless, removal of the mucocutaneous and arthritis items from SLEDAI did not substantially alter our results (online supplemental figure S6). These findings highlight the unmet needs in the management of lupus arthritis and mucocutaneous disease, as well as the possible beneficial role of novel biological agents following risk–benefit assessment.
Limitations of our study include its retrospective design prone to bias including that patients not meeting the targets might seek medical attention and perform tests more frequently, thus aiding the diagnosis of comorbidities. The cohort comprised exclusively of white participants, which could have accounted for the low prevalence of certain manifestations (eg, nephritis). Although the follow-up period reached the end of 2022, the use of licensed biological agents (belimumab) was still limited. Also, data on patient-reported outcomes were not available. One of the strengths is that the study was performed in two centres sharing common patient monitoring and treatment protocols. We studied a sufficiently large number of patients enrolled according to explicit inclusion criteria of disease activity/severity, who were monitored over a long observation period, thus enabling to capture a sufficient number of outcome events.
In conclusion, in patients with active (moderate-to-severe) SLE, remission (DORIS) and low disease activity (LLDAS) represent realistic goals associated with a reduction in irreversible organ damage and severe flares, therefore reinforcing their importance and value in clinical care. Attainment of the targets above specific observation time thresholds demonstrates high specificity for favourable prognosis, including significantly lower rates of adverse events and hospitalisation, with possible implications in treat-to-target implementation and clinical trial design. Arthritis and skin disease in SLE often lack sufficient therapeutic control highlighting the potential benefit of novel targeted agents.
Supplemental material
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplemental information. Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and data collection and analysis were approved by the ethics committees of the participating centres (protocol no. 13960/10-10-2018 and 516/2019/Oss/AOUFe). All patients gave informed consent upon inclusion in the respective registries.
Acknowledgments
We are thankful to the staff physicians and nurses of the Rheumatology Departments of the University Hospital of Heraklion and the University of Ferrara for providing care to the patients with SLE.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Josef S Smolen
Twitter @none, @george_bertsias
Contributors SP evaluated patients, completed data collection forms, performed data entry and drafted the manuscript. MN collected data and performed data entry and data curation. PG performed part of the statistical analysis. ES, AR, AM and NA evaluated patients and completed data collection forms. IF assisted with the electronic patient registry and data entry process. KP contributed to the study design, evaluated patients and completed data collection forms. MG and PS contributed to the study design and results interpretation and evaluated patients. DTB and AF contributed to the data analysis plan, interpretation of the results and to manuscript drafting. AB co-supervised the study, evaluated patients and completed data collection forms. GB conceived and co-supervised the study, evaluated patients, performed data curation and statistical analysis, and drafted the manuscript. GB acts as guarantor.
Funding The study received funding from the Research Account of the University of Crete (KA10210) and the Pancretan Health Association.
Competing interests ES received consulting fees from AstraZeneca out of the present work. AF reports honoraria and/or consulting fees from Lilly, Boehringer, Novartis, AbbVie, AstraZeneca, GSK, MSD, Pfizer, UCB, Amgen and Aenorasis, and support for attending meetings from UCB. MG has received fees for sponsored lectures from GSK and AstraZeneca. DTB reports unrestricted investigational grants from GSK, and honoraria and/or consulting fees from GSK, AstraZeneca and Pfizer. AB reports consulting fees from GSK. GB reports grants from GSK, AstraZeneca and Pfizer; honoraria and/or consulting fees from Lilly, Aenorasis, Novartis, AstraZeneca, GSK, SOBI and Pfizer; and participation in advisory boards from Novartis. The remaining authors declare no conflict of interest. One of the coauthors (DTB) is a member of the journal's editorial board.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.