Article Text

Abstract
Background: Glucocorticoids (GCs) are the mainstay of treatment for polymyalgia rheumatica (PMR). However, a substantial proportion of patients treated with GC may not achieve GC-free remission or may not be able to taper GC without experiencing flares.[1] It is estimated that almost 50% of patients experience a disease flare upon GC taper or discontinuation.[2,3] The clinical and economic burden of continuing GC in these patients could provide important insight into the potential value of steroid sparing therapy. Previous analyses defined inadequate response to GC/GC taper to include patients with comorbidities that may result from or worsen with GC use.[4] However, these occur at a high rate in this population and may not preclude use of GC in some patients. This analysis evaluates the clinical and economic outcomes in patients with PMR who are presumed to flare with GC use or relapse after discontinuation in a real-world setting.
Objectives: To estimate the clinical and economic outcomes of continuing GCs in patients with PMR who are IR to GC or unable to taper GC
Methods: A PMR inception cohort was derived using fee-for service Medicare claims data,[4] included patients aged ≥50 years with no prior history of PMR or giant cell arteritis who had 1) ≥1 inpatient or ≥2 outpatient claims for PMR (ICD-10-CM M35.3) ≥30 to <365 days apart, 2) prescription for GC (prednisone equivalent) 7.5–25 mg/day <30 days from 1st inpatient code or from 1st outpatient code to 30 days after 2nd code with GC dose ≥200 mg in first ≤30 days and continuous GC use ≥4 months 3) continuous enrollment ≥1 year prior to index and 4) ≥2 years follow-up. Index date was latter of the date the diagnosis or GC dose/use criteria was met; and was between 10/1/2016 and 12/31/2019. Patients with seropositive rheumatoid arthritis, other systemic rheumatic disease, solid organ transplant, multiple sclerosis, active treatment for malignancy or prescription for conventional immunomodulatory drugs [csIM (methotrexate [MTX], leflunomide, azathioprine)]/interleukin-6 receptor inhibitors during baseline (1 year prior to and including index) were excluded. Patients were divided into two groups: 1) IR-GC/GC taper, i.e., those with GC dose ≥7.5 mg/day at 6 months or persistent GC use >12 months (i.e., presumed flare) or relapse [GC use after discontinuation (>60-day gap)] or 2) non-IR-GC/GC taper (all others).
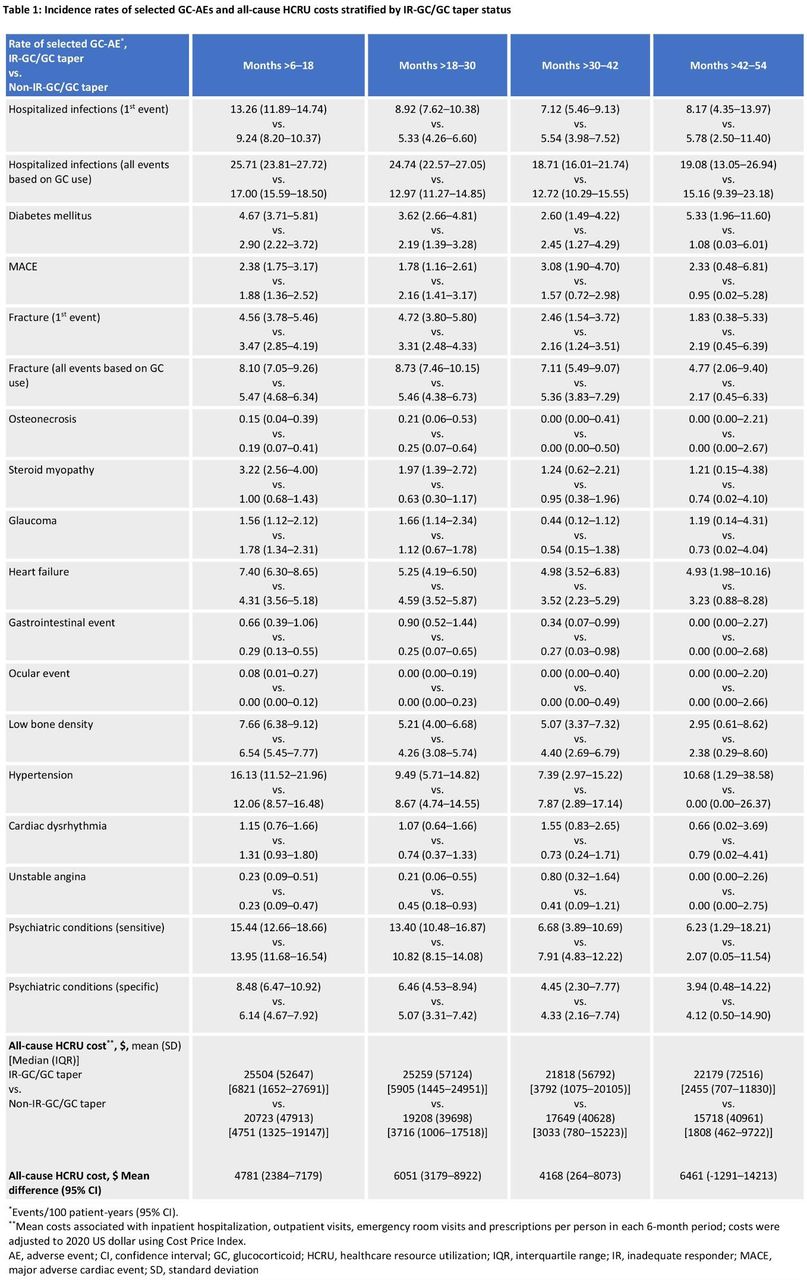
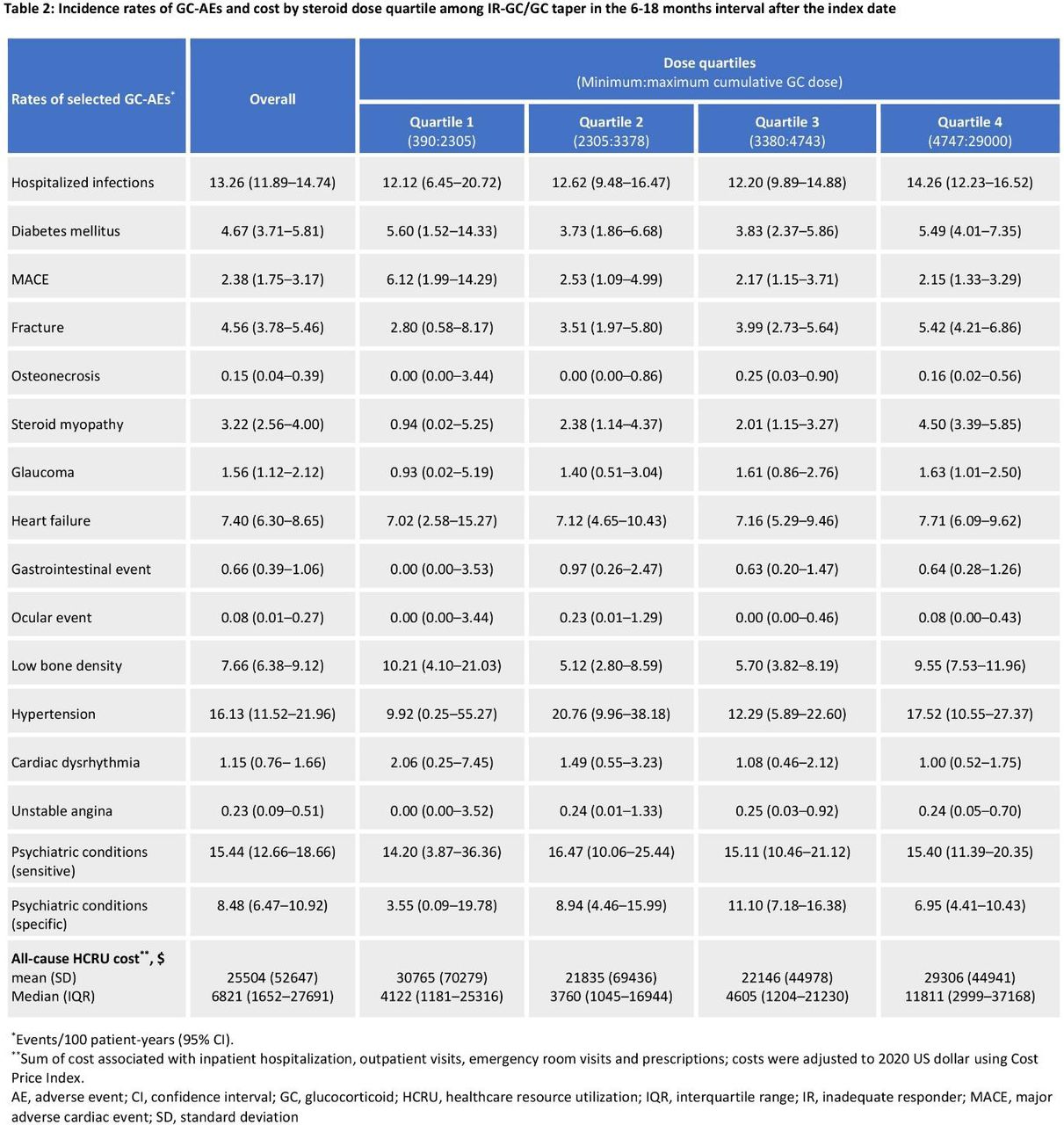
All-cause healthcare resource utilization (HCRU) costs, and incidence rate of GC-related adverse events (GC-AEs) as per ICD-10-CM diagnosis, drug, or procedure codes were reported beginning 6 months after index and updated at 6-months intervals. For hospitalized infections and fractures, repeat events were allowed; for all other AEs, only the 1st event was counted. Exact Poisson methods were used to estimate event rates per 100 patient-years and 95% confidence intervals. A subgroup analysis of the IR-GC/GC taper group estimated outcomes by cumulative GC dose quartiles, updated every 6 months.
Results: This analysis included 6054 patients with new onset PMR (65.4% females) with mean age 77.1 years. The rates of GC-AEs and all-cause HCRU costs were generally higher in the IR-GC/GC taper group vs. non-IR-GC/GC taper group in the months >6–18 and remained higher through months 42–54, except for osteonecrosis (Table 1). In the IR-GC/GC taper group, all-cause HCRU costs and most GC-AEs decreased over time. A GC dose-response relationship was noted between cumulative GC dose and most outcomes (Table 2).
Conclusion: The clinical and economic burden of continuing GCs in PMR patients with inability to taper GCs are considerable and may endure even after GC discontinuation. These results underscore the need for effective GC-sparing therapies for PMR to avoid/minimize the clinical and economic burden of long-term GCs.
REFERENCES: [1] Hutchings A, et al Arthritis Rheum 2007; 57:803–9.
[2] Salvarani C, et al Arthritis Rheum 2005; 53:33–38.
[3] Kremers HM, et al J Rheumatol 2005; 32:65–73
[4] Curtis J, et al Arthritis Rheumatol. 2023; 75 (suppl 9)


{kind=link}
{kind=link}
Acknowledgements: This study was funded by Sanofi and Regeneron Pharmaceuticals, Inc. Medical writing assistance was provided by Arohi Sarang M.Pharm. of Sanofi.
Disclosure of Interests: Jeffrey R Curtis AstraZeneca, Amgen, AbbVie, Bendcare, Genentech, GSK, Horizon, Janssen, Lilly, Novartis, Pfizer, Sanofi, Scipher, Setpoint, and UCB, AstraZeneca, Amgen, AbbVie, Bendcare, Genentech, GSK, Horizon, Janssen, Lilly, Novartis, Pfizer, Sanofi, Scipher, Setpoint, and UCB, Lita Araujo Employee of Sanofi and may hold stocks/stock options in the company, Stefano Fiore Employee of Sanofi and may hold stocks/stock options in the company, Sebastian E. Sattui Research funding from Bristol Myers Squibb Foundation Robert A. Winn Diversity in Clinical Trials Career Development Award; research support from AstraZeneca and GlaxoSmithKline (clinical trials) and consultant and participated in advisory boards for Sanofi and Amgen (all funds towards research support)., John H. Stone Consultant: Sanofi, Brandon Yip Employees of Sanofi and may hold stocks/stock options in the company, Kerri Ford Employee of Sanofi and may hold stocks/stock options in the company, Fenglong Xie: None declared.
- Tapering
- Glucocorticoids
- Economics
- Epidemiology
- Real-world evidence