Article Text

Abstract
Background: RA treatment aims for remission, but low disease activity (LDA) is an alternative goal if remission is unattainable. EULAR treatment recommendations in RA suggest that if patients do not respond to a first advanced therapy such as TNF- or IL-6 receptor inhibitor, then patients may receive an agent with another mode of action (MOA) or a second TNF- or IL-6 receptor inhibitor. Prior meta-analyses and economic evaluations found that switching to an advanced therapy with a different MOA may be more effective and less expensive than cycling through TNFis in patients with RA. Upadacitinib (UPA) is a recently approved JAK inhibitor, and its cost-effectiveness as second-line (2L) advanced treatment after discontinuing a TNFi, compared with other treatment strategies, has not yet been reported.
Objectives: To estimate the cost-effectiveness of 2L UPA compared with other treatment strategies, including TNFi cycling or switching to other advanced RA treatments, among patients with active RA who failed treatment with a TNFi in the UK
Methods: A cohort Markov model with 6-month cycles and lifetime horizon from age 55 was developed to estimate costs and effectiveness in quality-adjusted life years (QALY). Four health states were defined by DAS28-CRP: remission, LDA, moderate/high disease activity, and death. After first-line (1L) TNFi, the model evaluated a range of treatment strategies. Each strategy started with a treatment of interest (UPA, TNFis, baricitinib [BAR], tofacitinib [TOF], tocilizumab [TCZ], abatacept [ABT], and filgotinib [FLG]) and was followed by the sequence: TCZ → rituximab (RTX) → best supportive care. For the TCZ sequence, ABA was used as first follow-up treatment. Patients moved on to next treatment after entering moderate/high disease activity state on the current treatment. Transition probabilities were derived from phase 3 clinical trials for non-TNFi treatments, and from real-world studies for TNFis due to limited data. In a sensitivity analysis, DAS28 erythrocyte sedimentation rate (DAS28-ESR) efficacy data were substituted for DAS28-CRP. Costs of drug acquisition and administration, adverse events (AEs), monitoring, and hospitalization were estimated in 2021 GBP. Health state utilities were calculated from health assessment questionnaire (HAQ) scores using a published equation. We calculated total annual direct medical cost in the UK by weighing treatment costs based on current market shares and multiplying them by an estimate of the number of 2L patients with active RA.
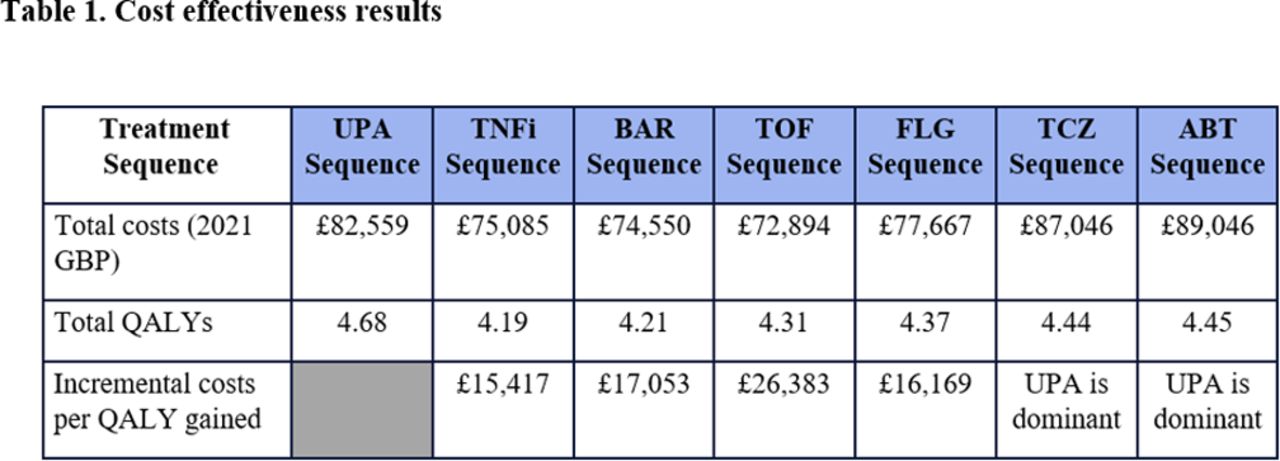
Results: The 2L UPA treatment sequence was cost-effective vs. sequences with TNFi cycling, BAR, TOF, and FLG at a £30,000/QALY threshold, and dominant against TCZ and ABT sequences (Table 1 and Figure 1). In the sensitivity analysis, UPA remained cost-effective vs. all comparators. The QALY gains of the UPA treatment sequence were driven by extended time in remission when being treated with UPA (3.16 years vs. 0.72 - 2.16 years for treatment with TNFi cycling or other treatment strategies). Higher acquisition costs for UPA mainly driven by longer time on treatment (£60,388 for UPA vs. £49,003 - £59,184 for TNFi cycling and other treatment strategies) were partially offset by lower administration costs (£3,849 for UPA vs. £4,772 - £11,247 for TNFi cycling and other treatment strategies) and lower AE, monitoring, and hospitalization costs due to longer time in remission with UPA. Total annual costs for 2L RA treatment in the UK were £756 million.
Conclusion: In this economic evaluation, switching to UPA after the 1L TNFi was associated with higher QALY compared with TNFi cycling and other treatment strategies, and was found to be cost-effective versus other treatment strategies based on a typical willingness-to-pay threshold of £30,000/QALY in the UK.
REFERENCES: NIL.


{kind=link}
{kind=link}
Acknowledgements: AbbVie funded this study and participated in the study design; study research; collection, analysis, and interpretation of data; and writing, reviewing, and approving of this publication. All authors had access to the data and participated in the development, review, and approval, and in the decision to submit this publication. No honoraria or payments were made for authorship.
Disclosure of Interests: Peter C. Taylor AbbVie, Biogen, Galapagos, Gilead, GlaxoSmithKline, Janssen, Lilly, Pfizer, Sanofi, Nordic Pharma, Fresenius, and UCB, Galapagos, Aditi Kadakia AbbVie, Yan Song Analysis Group Inc., Sander Strengholt AbbVie, Mirko Fillbrunn Analysis Group Inc., Anya Jiang Analysis Group Inc., Maya Buch AbbVie, Boehringer Ingelheim, Galapagos, Gilead, Lilly, and Pfizer, Gilead
- Targeted synthetic drugs
- biological DMARD
- Health services research
- Economics
- Remission